

Analysis of risk factors of children with severe hand-foot-mouth disease
-
摘要:
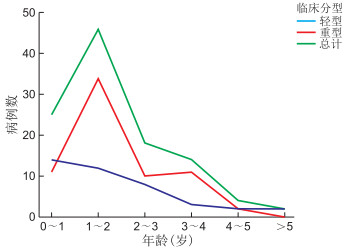
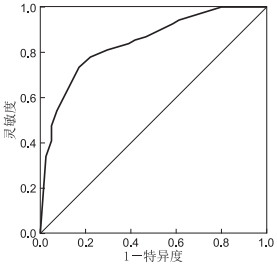
目的 观察重症手足口病(HFMD)患儿的主要实验室检测结果,寻找重症HFMD的危险因素并建立预测模型,为早期诊断、及时治疗提供帮助。 方法 选取2019年1—12月蚌埠医学院第一附属医院收治的HFMD患儿(包括临床诊断病例和确诊病例)为研究对象,分析临床症状、体征及主要的实验室指标,差异有统计学意义项进行多因素logistic回归分析,构建回归模型,绘制ROC曲线评估模型预测效果,使用SPSS 26.0统计学软件进行数据分析。 结果 通过分析109例(其中轻型41例,重症68例)HFMD患儿的临床资料发现,体温≥38.9 ℃(OR=2.943, 95% CI:1.099~7.884)、精神差(OR=5.899, 95% CI:2.130~16.339)、外周血白细胞升高(OR=4.386, 95% CI:1.420~13.541)、脑电图异常(OR=4.502,95% CI:1.714~11.821)为重症HFMD的独立危险因素(依次用X1、X2、X3、X4表示),预测模型的回归方程为Logit(P)=-2.893+1.079X1+1.775X2+1.478X3+1.504X4,该模型灵敏度为61.0%,特异度为83.8%,绘制ROC曲线对应的曲线下面积(AUC)为0.843,95% CI为0.768~0.917。 结论 体温≥38.9 ℃、精神差、外周血白细胞升高、脑电图异常为重症HFMD的独立危险因素,可构建预测HFMD重症的logistic回归模型。 Abstract:Objective To observe the primary laboratory examination results of children with severe hand-foot-mouth disease (HFMD), determine their risk factors and establish a prediction model to provide early diagnosis and timely HFMD treatment. Methods Children with HFMD (including clinical diagnosis cases and confirmed cases) were included in the study. They were admitted to the First Affiliated Hospital of Bengbu Medical College from January 2019 to December 2019. The clinical symptoms, signs and major laboratory indicators were analysed, and statistically significant terms were further processed via multifactor logistic regression to build a regression model. ROC curves were drawn to evaluate the predictive effect of the model. Data were analysed using SPSS 26.0 software. Results The clinical data of 109 HFMD cases (including 41 mild cases and 68 severe cases), showed that body temperature of ≥ 38.9 ℃ (OR=2.943, 95% CI: 1.099-7.884), poor spirit (OR=5.899, 95% CI: 2.130-16.339), increased peripheral blood white blood cells (OR=4.386, 95% CI: 1.420-13.541) and abnormal electroencephalogram (OR=4.502, 95% CI: 1.714-11.821) were independent risk factors for severe HFMD. The regression equation of the prediction model was Logit (P)=-2.893+1.079X1+1.775X2+1.478X3+1.504X4. The sensitivity of the model was 61.0%, and its specificity was 83.8%. The area under the curve corresponding to the ROC curve was 0.843 (95% CI: 0.768-0.917). Conclusion Body temperature of ≥ 38.9 ℃, poor spirit, increased peripheral blood white blood cells and abnormal electroencephalogram are independent risk factors for severe HFMD. These risk factors can be used to establish a predictive logistic regression model for severe HFMD. -
Key words:
- Hand-foot-mouth disease /
- Severe cases /
- Risk factors /
- Children
-
表 1 2组HFMD患儿临床资料比较[例(%)]
组别 例数 体温(℃) 皮疹部位(手、足、口、臀) 精神差 流涎 咳嗽、咳痰、肺部湿啰音等 紫绀、末梢循环差等 T < 37.5 37.5≤T < 38.5 38.5≤T < 39.5 单个部位 2个部位 3个部位 4个部位 轻型 41 2(4.9) 28(68.3) 11(26.8) 12(29.3) 11(26.8) 17(41.5) 1(2.4) 9(22.0) 21(51.2) 18(43.9) 0(0.0) 重症 68 4(5.9) 21(30.9) 43(63.2) 17(25.0) 15(22.1) 29(42.6) 7(10.3) 43(63.2) 47(69.1) 33(48.5) 0(0.0) χ2值 15.191 2.467 17.475 3.492 0.220 P值 0.001 0.497 < 0.001 0.062 0.639  下载: 导出CSV
下载: 导出CSV
表 2 2组HFMD患儿实验室指标比较(x ±s)
组别 例数 脑电图异常[例(%)] EV71IgM抗体[例(%)] CA16IgM抗体[例(%)] 合并其他病原菌[例(%)] WBC(×109/L) NE%(%) PA(mg/dL) GLU(mmol/L) 轻型 41 15(36.6) 3(7.3) 2(4.9) 10(24.4) 9.47±3.54 46.9±17.2 136.78±27.81 4.91±1.39 重症 68 52(76.5) 9(13.2) 13(19.1) 27(39.7) 11.68±3.94 55.1±15.6 132.74±34.08 5.99±1.70 统计量 17.180a 0.914a 3.253a 2.676a 8.620b 6.650b 0.412b 11.795b P值 < 0.001 0.339 0.071 0.102 0.004 0.011 0.522 0.001 组别 例数 CKMB(U/L) CR(μmol/L) UREA(mmol/L) ALT(U/L) AST(U/L) LDH(U/L) RBP(mg/L) 轻型 41 31.05±13.33 31.54±7.58 3.65±1.01 20.98±12.78 38.07±9.40 143.37±45.97 18.93±6.18 重症 68 32.25±16.45 29.81±7.83 3.57±0.95 17.82±9.34 36.31±9.92 223.91±39.29 17.85±5.14 统计量 0.156b 1.277b 0.161b 2.197b 0.841b 94.459b 0.957b P值 0.693 0.261 0.689 0.141 0.361 < 0.001 0.330 组别 例数 NLR[M(P25, P75)] PLR[M(P25, P75)] CK[M(P25, P75), U/L)] CRP[M(P25, P75), mg/L)] PCT[M(P25, P75), ng/mL)] 轻型 41 1.05(0.55, 1.84) 87.54(62.95, 104.74) 82.50(59.50, 105.50) 8.10(3.90, 17.90) 0.34(0.16, 0.77) 重症 68 1.80(1.11, 2.76) 85.86(64.57, 114.89) 86.00(58.00, 120.00) 14.80(5.03, 22.38) 0.35(0.18, 1.07) 统计量 -1.429c -1.486c -1.615c -1.454c -0.613c P值 0.153 0.137 0.106 0.146 0.540 注:a为χ2值,b为t值,c为U值。
下载: 导出CSV
表 3 重症HFMD患儿的多因素logistic回归分析
变量 B SE Wald χ2 P值 OR(95% CI) 体温≥38.9 ℃ 1.079 0.503 4.610 0.032 2.943(1.099~7.884) 精神差 1.775 0.520 11.658 0.001 5.899(2.130~16.339) WBC升高 1.478 0.575 6.605 0.010 4.386(1.420~13.541) 脑电图异常 1.504 0.493 9.328 0.002 4.502(1.714~11.821) 常量 -2.893 0.738 15.344 < 0.001 注:变量的赋值方法如下,发生重症HFMD是=2,否=1;体温≥38.9 ℃=2, < 38.9 ℃=1;精神差=2,精神一般或良好=1;白细胞计数>10×109/L=2,正常=1;脑电图异常=2,脑电图正常=1。
下载: 导出CSV
-
[1] 李兴旺. 手足口病诊疗指南(2018年版)[J]. 中华传染病杂志, 2018, 36(5): 257-263. doi: 10.3760/cma.j.issn.1000-6680.2018.05.001 [2] 成怡冰, 周崇臣, 宋春兰, 等. 危重型手足口病的影响因素分析及风险评分系统的建立研究[J]. 中国全科医学, 2018, 21(13): 1573-1579. doi: 10.3969/j.issn.1007-9572.2018.13.013 [3] QIU J, LU X, LIU X, et al. Derivation and validation of a mortality risk score for severe hand, foot and mouth disease in China[J]. Sci Rep, 2017, 7(1): 3371. doi: 10.1038/s41598-017-02658-4 [4] 张立霞, 马进. 重型手足口病临床特征及预警指标分析[J]. 蚌埠医学院学报, 2018, 43(5): 631-632, 636. https://www.cnki.com.cn/Article/CJFDTOTAL-BANG201805020.htm [5] 公共卫生科学数据中心. 手足口病[DB/OL]. [2020-05-10]. http://www.phsciencedata.cn/Share/ky_sjml.jsp?id=b9c93769-3e0f-413a-93c1-027d2009d8bc. [6] AW-YONG K L, NIKNADIA N M N, TAN C W, et al. Immune responses against enterovirus A71 infection: implications for vaccine success(Review)[J]. Rev Med Virol, 2019, 29(5): 2073. http://www.ncbi.nlm.nih.gov/pubmed/31369184 [7] 沈嬿, 陈中新, 胡建国, 等. EV71-IgM抗体检测在婴幼儿肠道病毒感染早期诊治和防控中的意义[J]. 中华全科医学, 2018, 16(5): 708-711. https://www.cnki.com.cn/Article/CJFDTOTAL-SYQY201805009.htm [8] 薛爱丽, 任祥欣, 贾静, 等. 101例手足口病重症病例流行学和临床特征分析[J]. 临床研究, 2019, 27(10): 6-8. https://www.cnki.com.cn/Article/CJFDTOTAL-LCYN201910005.htm [9] LI Z, CUI B, LIU X, et al. Virucidal activity and the antiviral mechanism of acidic polysaccharides against Enterovirus 71 infection in vitro[J]. Microbiol Immunol, 2020, 64(3): 189-201. doi: 10.1111/1348-0421.12763 [10] GAO E, WU S, XU Q, et al. Enterovirus type 71-immunized chicken egg yolk immunoglobulin has cross antiviral activity against coxsackievirus A16 in vitro[J]. Exp Ther Med, 2019, 18(1): 332-341. http://www.ingentaconnect.com/content/sp/etm/2019/00000018/00000001/art00041 [11] ROSENFELD-YEHOSHUA N, BARKAN S, ABU-KISHK I, et al. Hyperpyrexia and high fever as a predictor for serious bacterial infection (SBI) in children-a systematic review[J]. Eur J Pediatr, 2018, 177(3): 337-344. doi: 10.1007/s00431-018-3098-x [12] FLETCHER T, BLEEKER-ROVERS C, BEECHING N. Fever[J]. Medicine, 2017, 45(3): 177-183. doi: 10.1016/j.mpmed.2016.12.013 [13] ZHANG W, HUANG Z, HUANG M, et al. Predicting Severe Enterovirus 71-infected hand, foot, and mouth disease: cytokines and chemokines[J]. Mediators Inflamm, 2020. DOI: 10.1155/2020/9273241. [14] 何春卉. EV71感染手足口病患儿血清IL-6、IL-13水平变化及其原因[J]. 山东医药, 2017, 57(29): 78-80. doi: 10.3969/j.issn.1002-266X.2017.29.026 [15] LIN W, SU Y, JIANG M, et al. Clinical features for 89 deaths of hand, foot and mouth disease in Guangxi, China, 2014[J]. Int J Infect Dis, 2017, 64: 15-19. doi: 10.1016/j.ijid.2017.08.016 [16] 王猛, 孙丽敏, 刘洋, 等. 重症手足口病危险因素分析[J]. 泰山医学院学报, 2019, 40(10): 796-797. doi: 10.3969/j.issn.1004-7115.2019.10.033 [17] 张中馥, 张楠, 李清华, 等. 动态监测血清CRP、PCT水平对手足口病病情转归时的监测意义[J]. 河北医药, 2018, 40(13): 2030-2032. doi: 10.3969/j.issn.1002-7386.2018.13.029 [18] 李亚玲. NLR、PLR联合CRP检测对手足口病患儿的临床价值[J]. 检验医学与临床, 2018, 15(17): 2582-2584, 2588. doi: 10.3969/j.issn.1672-9455.2018.17.016 [19] 邓杨富, 欧阳辉, 陆桂宁. 手足口病患儿发生急性呼吸衰竭的预判性研究[J]. 海南医学院学报, 2018, 24(9): 942-944. https://www.cnki.com.cn/Article/CJFDTOTAL-HNYY201809012.htm [20] SUI M, HUANG X, LI Y, et al. Application and comparison of laboratory parameters for forecasting severe hand-foot-mouth disease using logistic regression, discriminant analysis and decision tree[J]. Clin Lab, 2016, 62(6): 1023-1031. http://europepmc.org/abstract/MED/27468564 -

 点击查看大图
点击查看大图

图(3) / 表(4)
计量
- 文章访问数: 608
- HTML全文浏览量: 372
- PDF下载量: 5
- 被引次数: 0
