

The prognostic value of SII, NLR, PLR and LMR in the stage of ⅠA-ⅡA2 cervical cancer
-
摘要:
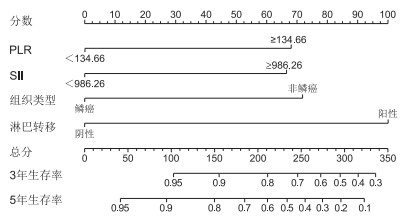
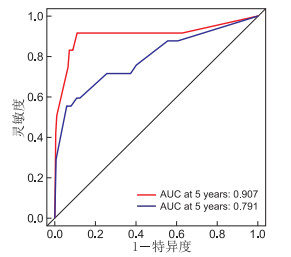
目的 探讨宫颈癌ⅠA2~ⅡA2期患者治疗前系统性免疫性炎症指数(SII)、中性粒细胞和淋巴细胞比值(NLR)、血小板与淋巴细胞比值(PLR)、淋巴细胞与单核细胞比值(LMR)对预后的预测价值。 方法 纳入2012年5月—2014年12月于蚌埠医学院第一附属医院初诊为宫颈癌ⅠA2~ⅡA2期的患者196例。求患者NLR、PLR、LMR、SII的最佳截断值,并分高、低值组。观察高、低值组4项指标与临床病理参数的关系。比较高、低值组生存时间(OS)差异。对影响预后的因素行单因素、多因素分析,并检验独立危险因素的预测效度,建立列线图。 结果 NLR与组织学类型和淋巴脉管间质浸润(LVSI)相关、PLR与组织学类型和肿瘤大小相关、SII与组织学类型相关,差异均有统计学意义(均P<0.05)。NLR、PLR、SII高值组及LMR低值组的OS 3.5年更短,差异均有统计学意义(均P<0.05)。PLR、SII、组织学类型、淋巴结转移是影响OS的独立危险因素(均P<0.05)。预测效度:PLR>SII>淋巴结转移>组织学类型(AUC:73.2%>71.9%>65.1%>37.0%)。列线图预测准确度较高(OS 3年、OS 5年AUC为90.7%、79.1%)。 结论 治疗前PLR、SII值可成为术前预测ⅠA2~ⅡA2期宫颈癌患者预后的可靠指标。 -
关键词:
- 系统性免疫性炎症指数 /
- 中性粒细胞和淋巴细胞比值 /
- 血小板与淋巴细胞比值 /
- 淋巴细胞与单核细胞比值 /
- 宫颈癌
Abstract:Objective To investigate the prognostic value of systemic immune inflammatory index (SⅡ), neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), and lymphocyte to monocyte ratio (LMR) in patients with cervical cancer of stage ⅠA-ⅡA2 before treatment. Methods 196 patients with cervical cancer of stage ⅠA2-ⅡA2 who were initially diagnosed in the First Affiliated Hospital of Bengbu Medical College from May 2012 to December 2014 were included. The Cut off values of NLR, PLR, LMR and SⅡ were calculated and divided into high and low value groups.The relationship between the four indexes and clinicopathological parameters in the high and low value groups were observed. The difference in overall survival between high and low value groups were compared. Univariate and multivariate analyses were performed to assess the predictive validity of independent risk factors, and establish a nomogram. Results NLR was correlated with histological type and lymphatic vascular stromal infiltration, PLR was correlated with histological type and tumor size, and SⅡ was correlated with histological type, with statistically significant difference respectively (all P < 0.05). The high value group of NLR, PLR and SⅡ and the low value group of LMR had shorter OS, and the difference was statistically significant (all P < 0.05). PLR, SⅡ, histological type and lymph node metastasis were independent risk factors for OS (all P < 0.05). Predictive validity: PLR>SⅡ>lymph node metastasis>the histological type (AUC: 73.2%>71.9%>65.1%>37.0%). The accuracy of the nomogram was high (OS3/OS5 AUC: 90.7%/79.1%). Conclusion The value of PLR and SⅡ before treatment can be reliable indicators to predict the prognosis of patients with stage ⅠA2~ⅡA2 cervical cancer. -
表 1 4项炎症指标高、低值组与患者临床病理特征的关系(例)
项目 SII Z值 P值 NLR Z值 P值 PLR Z值 P值 LMR Z值 P值 高值 低值 高值 低值 高值 低值 高值 低值 年龄(岁) <47 32 63 -0.839 0.401 46 52 -0.647 0.518 46 52 -1.592 0.111 46 49 -0.122 0.903 ≥47 27 74 45 53 38 60 53 48 FIGO分期 ⅠA2~ⅠA2期 46 103 -0.420 0.679 74 75 -1.517 0.129 62 87 -0.881 0.378 73 76 0.754 0.452 ⅡA1~ⅡA2期 13 34 17 30 22 25 26 21 组织学类型 鳞癌 43 122 -2.840 0.010 71 94 -2.006 0.045 64 101 -2.583 0.010 85 81 -0.455 0.650 非鳞癌 16 15 20 11 20 11 14 16 病理级别 ≤2级 15 39 -0.440 0.660 66 76 -0.033 0.974 60 82 -0.509 0.611 70 72 0.549 0.583 >2级 44 98 25 29 24 30 29 2 肿瘤大小(cm) ≤4 27 70 -0.680 0.501 43 54 -1.004 0.315 34 63 -2.032 0.042 74 64 -1.343 0.181 >4 32 67 48 51 50 49 25 33 淋巴结转移 阴性 43 112 -1.401 0.160 70 85 -0.819 0.413 58 87 -0.629 0.529 80 75 -0.597 0.551 阳性 16 25 21 20 16 25 19 22 浸润程度 <1/2肌层 17 36 -0.369 0.720 25 28 -0.187 0.852 25 28 -0.652 0.514 29 24 -0.715 0.476 ≥1/2肌层 42 101 66 77 59 84 70 73 LVSI 阴性 54 121 -0.659 0.509 86 89 -2.338 0.019 76 99 -0.515 0.607 89 86 -0.279 0.781 阳性 5 16 5 16 8 13 10 11  下载: 导出CSV
下载: 导出CSV
表 2 4项炎症指标高、低值组术后OS比较
指标 组别 例数 OS 3年(%) OS 5年(%) 中位生存时间 Log-rank检验 χ2值 P值 SII 高值组 59 83.1 72.7 64 21.552 < 0.001 低值组 137 97.8 93.3 66 NLR 高值组 91 75.2 71.8 64 14.896 0.001 低值组 105 94.8 94.8 66 PLR 高值组 84 88.1 77.3 65 13.660 < 0.001 低值组 112 97.3 94.5 66 LMR 高值组 99 97.0 94.8 66 9.684 0.020 低值组 97 79.3 74.6 64
下载: 导出CSV
表 3 预后影响因素单因素分析
项目 B SE Wald χ2 P值 HR值 95% CI NLR -1.289 0.038 28.101 < 0.001 1.208 1.121~1.301 PLR -1.384 0.002 35.173 < 0.001 1.011 1.008~1.015 LMR 1.138 0.104 6.846 0.009 0.762 0.621~0.934 SII -1.487 0.000 33.805 < 0.001 1.001 1.000~1.001 年龄 0.058 0.018 10.108 0.018 1.060 1.022~1.099 FIGO分期 0.513 0.356 2.118 0.146 1.670 0.831~3.358 组织类型 1.564 0.348 24.538 < 0.001 4.777 2.416~9.445 病理级别 0.752 0.347 4.917 0.027 2.120 1.074~4.184 肿瘤大小 0.897 0.339 7.548 0.006 2.452 1.261~4.768 淋巴转移 1.226 0.341 14.523 < 0.001 3.406 1.744~6.652 浸润深度 0.232 0.403 0.333 0.564 1.261 0.572~2.780 LVSI 0.038 0.532 0.005 0.943 1.039 0.366~2.946
下载: 导出CSV
表 4 预后影响因素多因素分析
项目 B SE Wald χ2 P值 HR值 95% CI PLR -0.924 0.003 24.146 0.009 1.007 1.002~1.013 SII -0.841 0.001 23.571 0.029 1.001 1.000~1.001 组织类型 1.129 0.392 17.143 0.002 3.327 1.542~7.177 淋巴转移 1.333 0.454 11.760 < 0.001 5.776 2.373~14.061
下载: 导出CSV
-
[1] WILD C P, WEⅡDERPASS E, STEWART B W. World cancer report: cancer research for cancer prevention[M]. Lyon: International Agency for Research on Cancer, 2020. [2] HUANG H, LIU Q, ZHU L, et al. Prognostic value of preoperative systemic immune-inflammation index in patients with cervical cancer[J]. Sci Rep, 2019, 9(1): 87-108. doi: 10.1038/s41598-018-36442-9 [3] TEOH D G K, ISAKSSON V R, MONU M, et al. The predictive value of neutrophil to lymphocyte ratio and platelet to lymphocyte ratio in determining cervical cancer stage[J]. Gynecol Oncol, 2017, 145(3): 83. http://www.sciencedirect.com/science?_ob=ShoppingCartURL&_method=add&_eid=1-s2.0-S0090825817304110&originContentFamily=serial&_origin=article&_ts=1498985259&md5=e0eb81f6f3ccd574b01e6afb6d084274 [4] HAMILTON T, STEPHEN P D, JALAL H, et al. Prognostic value of changes in neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and lymphocyte-to-monocyte ratio (LMR) for patients with cervical cancer undergoing definitive chemoradiotherapy (dCRT)[J]. Clinca Chimica Acta, 2020, 510(5): 711-716. http://www.sciencedirect.com/science/article/pii/S000989812030440X [5] 周晖, 刘昀昀, 罗铭, 等. 《2020 NCCN子宫颈癌临床实践指南(第1版)》解读[J]. 中国实用妇科与产科杂志, 2020, 36(2): 131-138. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGSF202002011.htm [6] 解秀珍. ⅠB-ⅡA期宫颈癌患者宫旁组织浸润的相关因素及腺癌与鳞癌的预后比较[D]. 济南: 山东大学, 2017. [7] KAILASH N, MING Y L, SRINIVAS K-C, et al. Redistribution of cervix cancer patients from FIGO 2009 to FIGO 2018 staging following incorporation of medical imaging[J]. Int J Gynecol Cancer, 2019, 17(4): 1-8. http://www.researchgate.net/publication/336989640_Redistribution_of_Cervix_Cancer_Patients_from_FIGO_2009_to_FIGO_2018_Staging_Following_Incorporation_of_Medical_Imaging [8] RICHA S, MOHAMMAD A, VARSHA S, et al. M2 polarization of macrophages by Oncostatin M in hypoxic tumor microenvironment is mediated by mTORC2 and promotes tumor growth and metastasis[J]. Cytokine, 2019, 118(6): 130-143. http://www.sciencedirect.com/science?_ob=ShoppingCartURL&_method=add&_eid=1-s2.0-S1043466618301182&originContentFamily=serial&_origin=article&_ts=1522773976&md5=5b2cc6f4c76375a499cc5439562552d4 [9] VITKAUSKAITE A, URBONIENE D, CELIESITUE J, et al. Circulating inflammatory markers in cervical cancer patients and healthy controls[J]. J Immunotoxicol, 2020, 17(1): 105-109. doi: 10.1080/1547691X.2020.1755397 [10] 王金凤, 李琛, 黄康榕, 等. 术前中性粒细胞和淋巴细胞比值、单核细胞和淋巴细胞比值与宫颈癌患者临床病理特征的相关性[J]. 兰州大学学报(医学版), 2019, 45(5): 25-29. https://www.cnki.com.cn/Article/CJFDTOTAL-LZYX201905008.htm [11] YUDA P, AGHA B, FIRDY L, et al. Pretreament neutrophi-to-lymphocyte ratio(NLR) and platelt-to-lymphocyte ratio(PLR) as a predicitive value of hematological markers in cervical cancer[J]. Asian Pac J Cancer Prew, 2019, 20(3), 863-868. doi: 10.31557/APJCP.2019.20.3.863 [12] ZHU M, FENG M, HE F, et al. Pretreatment neutrophil-lymphocyte and platelet-lymphocyte ratio predict clinical outcome and prognosis for cervical Cancer[J]. Clinica Chimica Acta, 2018, 483(5): 296-302. [13] CHEN L, ZHANG F, SHENG X, et al. Peripheral platelet/lymphocyte ratio predicts lymph node metastasis and acts as a superior prognostic factor for cervical cancer when combined with neutrophil: lymphocyte[J]. Medicine, 2016, 95(32): e4381. doi: 10.1097/MD.0000000000004381 [14] JI Y F, WANG H Y. Prognostic prediction of systemic immune-inflammation index for patients with gynecological and breast cancers: a meta-analysis[J]. World J Surg Oncol, 2020, 18(1): 847-860. http://www.researchgate.net/publication/343520941_Prognostic_prediction_of_systemic_immune-inflammation_index_for_patients_with_gynecological_and_breast_cancers_a_meta-analysis/download [15] GAO Y, GUO W, CAI S, et al. Systemic immune-inflammation index (SⅡ) is useful to predict survival outcomes in patients with surgically resected esophageal squamous cell carcinoma[J]. J Cancer, 2019, 10(14): 3188-3196. doi: 10.7150/jca.30281 [16] CHAO B, JU X, ZHANG L, et al. A novel prognostic marker systemic inflammation response index (SIRI) for operable cervical cancer patients[J]. Front Oncol, 2020, 10(1): 766. http://www.researchgate.net/publication/341348990_A_Novel_Prognostic_Marker_Systemic_Inflammation_Response_Index_SIRI_for_Operable_Cervical_Cancer_Patients [17] HOLUB K, BIETE A. Impact of systemic inlammation biomarkers on the survival outcomes of cervical cancer patients[J]. Clin Transl Oncol, 2019, 21(7): 836-844. doi: 10.1007/s12094-018-1991-4 [18] WU J, CHEN M, LIANG C, et al. Prognostic value of the pretreament neutrophi-to-lymphocyte ratio in cervical cancer: A meta-analysis and systematic review[J]. Oncotarget, 2017, 8(8): 13400-13412. doi: 10.18632/oncotarget.14541 [19] KOZASA K, MABUCHI S, KOMURA N, et al. Comparison of clinical utilities of the platelet count and platelet-lymphocyte ratio for predicting survival in patients with cervical cancer: a single institutional study and literature review[J]. Oncotarget, 2017, 8(33): 55394-55404. doi: 10.18632/oncotarget.19560 [20] Paul D S, Trinh H, Hyder J, et al. Prognostic value of changes in neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and lymphocyte-to-monocyte ratio (LMR) for patients with cervical cancer undergoing definitive chemoradiotherapy (dCRT)[J] Clinica Chimica Acta, 2020, 510(11): 711-716. http://www.sciencedirect.com/science/article/pii/S000989812030440X -

 点击查看大图
点击查看大图

图(3) / 表(4)
计量
- 文章访问数: 817
- HTML全文浏览量: 477
- PDF下载量: 9
- 被引次数: 0
