

Multivariate analysis of prognosis and nomogram construction of cystadenocarcinoma based on SEER database
-
摘要:
目的 通过研究膀胱腺癌(adenocarcinoma of the bladder,ACB)患者独立预后危险因素,建立可以个体化预测膀胱腺癌患者生存预后的列线图模型。 方法 通过收集SEER数据库中2004—2015年诊断为膀胱腺癌患者的临床资料进行筛选,共纳入符合研究条件的腺癌患者659例进行回顾性分析研究,采用Empower Stat软件对所有变量进行COX单因素回归分析,将P < 0.05的变量纳入COX多因素回归分析,使用R语言将COX多因素回归分析中的独立预后危险因素构建成生存列线图模型,运用Bootstrap法进行1 000次等量有放回重复采样对模型进行验证,采用C-index和绘制列线图校准曲线来验证模型的准确性。 结果 年龄>70岁、肿瘤直径>3 cm、未行手术治疗、T3期、T4期、N1期、N2期、M1期为影响患者生存时间的独立危险因素。建立的列线图校准曲线与理想曲线一致性较高,并采用C-INDEX(一致性指数)进行验证,C-INDEX指数为0.74,经内部验证后具有较高的适用性与准确性。 结论 本研究通过SEER数据库确定了ACB患者预后的独立危险因素,并且建立了国内外首个可以进行个体化预测ACB患者生存预后的列线图模型,从而指导临床医师选择合理的治疗方案,并对不同患者预后进行精准的个体化评估。 Abstract:Objective This study aimed to establish a nomogram model that can individually predict the prognosis of patients with bladder adenocarcinoma (ACB) by studying the independent prognostic risk factors. Methods Clinical data of patients diagnosed with ACB from 2004 to 2015 in the SEER database were collected for screening. A total of 659 patients with adenocarcinoma who met the study conditions were included for retrospective analysis. COX univariate regression analysis was performed on all variables using Empower stat software, and P < 0.05 was analysed. Variables of 0.05 were included in COX multivariate regression analysis. Independent prognostic risk factors determined in COX multivariate regression analysis were constructed into a survival nomogram model using R language. The bootstrap method was used to perform 1 000 times of equal number of repeated sampling to verify the model. Results Age > 70 years, tumour size>3 cm, T3, T4, N1, N2 and M1 were independent risk factors affecting the survival time of patients. The established alignment curve of the nomogram has a high consistency with the ideal curve and high applicability and accuracy after internal verification. Conclusion In this study, the seer database was used to determine the independent risk factors for the prognosis of ACB patients, and the first nomogram model was established to individually predict the survival prognosis of ACB patients and guide clinicians in selecting reasonable treatment options and conducting accurate individualised assessment of the prognosis of different patients. -
Key words:
- Adenocarcinoma of the bladder /
- SEER database /
- Nomogram /
- Prognosis
-

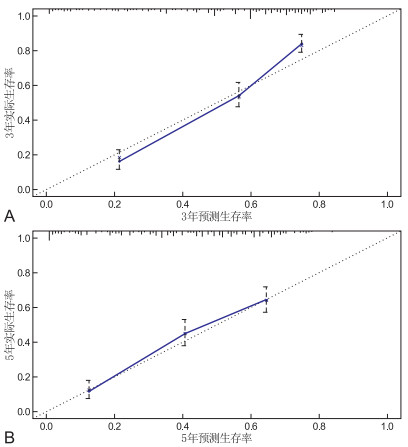
图 2 列线图校准曲线
注:A为3年列线图校准曲线,B为5年列线图校准曲线。黑色曲线代表模型实际预测结果与理想预测结果完全一致,蓝色实线为模型实际预测性能,与X轴黑色垂直线为95% CI。
表 2 变量赋值表
项目 变量 赋值 年龄 < 50岁=1;50~59岁=2;60~69岁=3;70~79岁=4; > 80岁=5 人种 以黑种人为参照设置哑变量 哑变量X1:白种人=1, 黑种人、亚太人=0;哑变量X2:亚太人=1,白种人、亚太人=0 性别 以男性为参照设置哑变量 哑变量X1:女=1,男=0 位置 以膀胱/膀胱三角为参照设置哑变量 哑变量X1:前/侧/后璧=1,膀胱/膀胱三角、脐尿管/顶壁、其他区域=0;哑变量X2:脐尿管/顶壁=1,前/侧/后璧、脐尿管/顶壁、其他区域=0;哑变量X3:其他区域=1前/侧/后璧、脐尿管/顶壁、前/侧/后璧=0 分级 Ⅰ级=1;Ⅱ级=2;Ⅲ级=3;Ⅳ级=4 病理分型 以混合型腺癌为参照设置哑变量 哑变量X1:透明细胞癌=1,印戒细胞癌、黏液腺癌、混合型腺癌=0;哑变量X2:印戒细胞癌=1,透明细胞癌黏液腺癌、混合型腺癌=0;哑变量X3:黏液腺癌=1,印戒细胞癌、印戒细胞癌、混合型腺癌=0 手术 手术=1;未手术=2 放疗 放疗=1;未放疗=2 化疗 化疗=1;未化疗=2 肿瘤大小 < 3 cm=1; > 3 cm=2 T分期 T1=1;T2=2;T3=3;T4=4 N分期 N0=1;N1=2;N3=3 M分期 M0=1;M2=2 生存情况 生存=1;死亡=2  下载: 导出CSV
下载: 导出CSV
表 1 659例膀胱腺癌患者一般临床资料
项目 例(%) 项目 例(%) 年龄(岁) 手术 < 50 108(16.39) 是 644(97.72) 50~59 137(20.79) 否 15(2.28) 60~69 157(23.82) 放疗 70~79 149(22.61) 是 81(12.29) > 80 108(16.39) 否 578(87.71) 人种 化疗 黑种人 84(12.75) 是 473(71.78) 白种人 520(78.91) 否 186(28.22) 亚太人 55(8.35) 肿瘤大小(cm) 性别 < 3 262(39.76) 男性 399(60.55) > 3 397(60.24) 女性 260(39.45) T分期 位置 T1 116(17.60) 膀胱/膀胱三角 77(11.68) T2 213(32.32) 前/侧/后璧 129(19.58) T3 222(33.69) 脐尿管/顶壁 259(39.30) T4 108(16.39) 其他区域 194(29.43) N分期 分级 N0 536(81.34) Ⅰ 53(8.04) N1 62(9.41) Ⅱ 246(37.33) N2 59(8.95) Ⅲ 251(38.09) N3 2(0.30) Ⅳ 109(16.54) M分期 病理分型 M0 597(90.59) 混合型腺癌 370(56.15) M1 62(9.41) 透明细胞癌 27(4.10) 印戒细胞癌 105(15.93) 黏液腺癌 157(23.82)
下载: 导出CSV
表 3 COX单因素回归分析
项目 HR(95%CI) P值 项目 HR(95%CI) P值 年龄(岁) 手术 < 50 1(参照值) 是 1(参照值) 50~59 1.1(0.8~1.6) 0.478 否 3.3(1.8~6.0) < 0.001 60~69 1.1(0.8~1.5) 0.693 放疗 70~79 1.7(1.2~2.4) 0.001 是 1(参照值) > 80 2.1(1.5~3.0) < 0.001 否 0.6(0.4~0.8) < 0.001 性别 化疗 男性 1(参照值) 是 1(参照值) 女性 1.0(0.8~1.3) 0.869 否 1.4(1.2~1.8) < 0.001 种族 肿瘤大小(cm) 黑人 1(参照值) < 3 1(参照值) 白人 0.9(0.6~1.1) 0.287 > 3 1.5(1.2~1.9) < 0.001 亚太人 0.6(0.4~1.0) 0.057 T分期 位置 T1 1(参照值) 膀胱/膀胱三角 1(参照值) T2 1.4(1.0~1.9) 0.073 前/侧/后璧 0.9(0.7~1.3) 0.700 T3 1.4(1.0~1.9) 0.051 脐尿管/顶壁 0.5(0.4~0.7) < 0.001 T4 5.4(3.8~7.7) < 0.001 其他区域 1.1(0.8~1.6) 0.421 N分期 分级 N0 1(参照值) Ⅰ 1(参照值) N1 2.4(1.8~3.3) < 0.001 Ⅱ 1.2(0.7~1.9) 0.515 N2 3.7(2.7~5.1) < 0.001 Ⅲ 2.6(1.6~4.1) < 0.001 N3 2.6(0.7~10.5) 0.176 Ⅳ 2.3(1.4~3.8) 0.001 M分期 病理分型 M0 1(参照值) 混合型腺癌 1(参照值) M1 3.1(2.3, 4.2) < 0.001 透明细胞癌 1.3(0.8~2.1) 0.315 印戒细胞癌 1.9(1.5~2.5) < 0.001 黏液腺癌 0.8(0.6~1.0) 0.036
下载: 导出CSV
表 4 COX多因素回归分析
项目 类别 B SE Wald χ2 P值 HR值 95%CI 年龄 < 50 50~59 0.189 0.247 1.048 0.805 1.04 0.72~1.51 60~69 0.187 1.086 1.225 0.278 1.22 0.84~1.76 70~79 0.184 3.312 1.840 < 0.001 1.83 1.28~2.63 > 80 0.195 4.687 2.491 < 0.001 2.49 1.70~3.65 病理分型 混合型腺癌 透明细胞癌 0.271 0.120 1.033 0.905 1.03 0.60~1.75 印戒细胞癌 0.152 0.267 1.042 0.789 1.04 0.77~1.40 黏液腺癌 0.148 -2.198 0.721 0.028 0.72 0.53~0.96 手术 是 否 0.332 3.682 3.399 < 0.001 3.39 1.77~6.52 肿瘤大小 < 3 cm > 3 cm 0.117 2.595 1.355 0.009 1.35 1.07~1.70 T分期 T1 T2 0.177 1.719 1.360 0.085 1.35 0.95~1.91 T3 0.188 3.067 1.779 < 0.001 1.77 1.23~2.57 T4 0.217 6.675 4.266 < 0.001 4.26 2.78~6.53 N分期 N0 N1 0.173 1.930 1.396 0.041 1.41 1.00~1.98 N2 0.184 4.180 1.396 < 0.001 2.16 1.51~3.10 N3 0.727 0.748 1.723 0.454 1.72 0.41~7.15 M分期 M0 M1 0.172 4.596 2.152 < 0.001 2.15 1.55~2.98 注: 以上表格中的HR均以第一组变量为参照值。
下载: 导出CSV
-
[1] NING J Z, YU W M, CHENG F, et al. MiR-425 promotes migration and invasion in bladder cancer by targeting Dickkopf 3[J]. J Cancer, 2020, 11(12): 3424-3432. doi: 10.7150/jca.40233 [2] 江明友, 万明发, 洪钟亮. 尿液BLCA-4与BLCA-1水平在膀胱癌诊断及复发检测中的价值[J]. 中华全科医学, 2018, 16(4): 570-572. https://www.cnki.com.cn/Article/CJFDTOTAL-SYQY201804019.htm [3] MOSCHINI M, D'ANDREA D, KORN S, et al. Characteristics and clinical significance of histological variants of bladder cancer[J]. Nat Rev Urol, 2017, 14(Suppl 2): 651-668. http://www.nature.com/articles/nrurol.2017.125.pdf [4] 江明友, 万明发, 洪钟亮. 尿液BLCA-4与BLCA-1水平在膀胱癌诊断及复发检测中的价值[J]. 中华全科医学, 2018, 16(4): 570-572. https://www.cnki.com.cn/Article/CJFDTOTAL-SYQY201804019.htm [5] VASUDEVAN G, BISHNU A, SINGH B M K, et al. Bladder adenocarcinoma: a persisting diagnostic dilemma[J]. J Clin Diagn Res, 2017, 11(3): ER01-ER04. http://jcdr.net/articles/PDF/9536/24590_CE[Ra1]_F(DK)_PF1(SY_RK)_PFA(P)_PF2(P_NESY).pdf [6] SIEGEL REBECCA L, MILLER KIMBERLY D, JEMAL AHMEDIN. Cancer statistics, 2019[J]. CA Cancer J Clin, 2019, 69(1): 7-34. doi: 10.3322/caac.21551 [7] 郭晓雪, 刘云鹤, 李文涛, 等. 膀胱原发性腺癌1例报告并文献复习[J]. 亚太传统医药, 2018, 14(7): 124-125. https://www.cnki.com.cn/Article/CJFDTOTAL-YTCT201807045.htm [8] 许晖阳, 王道虎. 膀胱腺癌的诊治进展[J]. 国际泌尿系统杂志, 2017, 37(2): 271-273. doi: 10.3760/cma.j.issn.1673-4416.2017.02.032 [9] SZARVAS T, MÔDOS O, NIEDWOROK C, et al. Clinical, prognostic, and therapeutic aspects of urachal carcinoma-A comprehensive review with meta-analysis of 1, 010 cases[J]. Urol Oncol, 2016, 34(9): 388-398. doi: 10.1016/j.urolonc.2016.04.012 [10] 顾伟平, 徐耀庭, 李杜渐, 等. 二次电切结合吉西他滨膀胱灌注化疗治疗肌层浸润性膀胱癌[J]. 中国临床研究, 2018, 31(9): 1215-1219. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGCK201809016.htm [11] KIM M J, KIM Y S, OH S Y, et al. Retrospective analysis of palliative chemotherapy for the patients with bladder adenocarcinoma: Korean Cancer Study Group Genitourinary and Gynecology Cancer Committee[J]. Korean J Intern Med, 2018, 33(2): 383-390. doi: 10.3904/kjim.2015.162 [12] TSIRONIS G, BAMIAS A. Treating bladder adenocarcinoma[J]. Transl Androl Urol, 2018, 7(Suppl 6): S699-S701. [13] 翟天元, 罗彬杰, 贾占奎, 等. 53例膀胱腺癌的临床特征及预后相关因素分析[J]. 实用医学杂志, 2018, 34(14): 2393-2397. doi: 10.3969/j.issn.1006-5725.2018.14.028 [14] NATALE C, LEINWAND Z G, CHIANG J, et al. Reviewing the demographic, prognostic, and treatment factors of primary adenocarcinoma of the bladder: a seer population-based study[J]. Clin Genitourin Cancer, 2019, 17(5): 380-388. doi: 10.1016/j.clgc.2019.06.010 [15] JIN D, QIU S, JIN K, et al. Signet-Ring cell carcinoma as an independent prognostic factor for patients with urinary bladder cancer: a population-based study[J]. Front Oncol, 2020, 10: 653. doi: 10.3389/fonc.2020.00653 [16] ZHOU Z, KINSLOW C J, WANG P, et al. Clear cell adenocarcinoma of the urinary bladder is a glycogen-rich tumor with poorer prognosis[J]. Clin Med, 2020, 9(1): 138. http://www.researchgate.net/publication/338379928_Clear_Cell_Adenocarcinoma_of_the_Urinary_Bladder_Is_a_Glycogen-Rich_Tumor_with_Poorer_Prognosis [17] WANG J W, WU Y, HE W Y, et al. Nomogram for predicting overall survival of patients with bladder cancer: A population-based study[J]. Int J Biol Markers, 2020, 35(2): 29-39. doi: 10.1177/1724600820907605 [18] CUMBERBATCH M G K, JUBBER I, BLACK P C, et al. Epidemiology of bladder cancer: a systematic review and contemporary update of risk factors in 2018[J]. Eur Urol, 2018, 74(6): 784-795. doi: 10.1016/j.eururo.2018.09.001 -

 点击查看大图
点击查看大图

图(2) / 表(4)
计量
- 文章访问数: 374
- HTML全文浏览量: 183
- PDF下载量: 8
- 被引次数: 0
