

Current situation and influencing factors of anticoagulant therapy for patients with atrial fibrillation in county hospitals based on data mining
-
摘要:
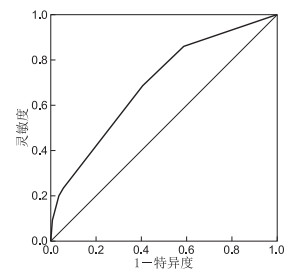
目的 本研究基于多中心房颤住院患者的抗凝数据分析挖掘,了解我国东部地区县级医院房颤患者抗凝治疗现状和影响因素,为未来县级房颤患者抗凝提供优化依据,以期预防房颤患者卒中发生从而降低疾病负担。 方法 通过回顾性分析我国东部3家县级医院2018—2019年2 452例房颤住院患者的诊疗及处方数据,描述分析县级医院房颤患者基本情况,并从不同维度分组抗凝差异性比较及县级医院房颤患者抗凝治疗的影响因素。 结果 3家县级医院整体抗凝率为49.96%,CHA2DS2-VASc评分≥2分的房颤患者抗凝率为50.4%,抗凝率在不同入院年份、入院科别、年龄组、合并疾病和出血风险分组比较,差异有统计学意义(均P<0.05);构建CRT决策树模型分析县级医院房颤抗凝的影响因素,最终纳入房颤主诊断、冠心病、心力衰竭、合并疾病数量、入院科别、卒中风险和出血风险、CHA2DS2-VASc评分等15个变量,模型准确度为65.0%,ROC曲线下面积为0.70。 结论 我国东部部分县级医院高卒中风险房颤患者的抗凝率有一定提升,但与三级医院比较仍有较大提升空间,此外,县级医院医生的抗凝规范性有待提升,未来仍需加强县级医院医生在房颤抗凝治疗方面的培训。 Abstract:Objective To understand the current situation and influencing factors of anticoagulant therapy for patients with atrial fibrillation in county-level hospitals in eastern China, and to optimise anticoagulant treatment, prevent stroke and reduce disease burden of these patients in the future. Methods Through retrospective analysis of the diagnosis, treatment and prescription data of 2 452 patients with atrial fibrillation in three county-level hospitals in eastern China from 2018 to 2019, the basic situation of these patients was described and analysed, and the differences of anticoagulation in different dimensions and the influencing factors of anticoagulation treatment were compared. Results The overall anticoagulation rate of three county-level hospitals was 49.96%, and the anticoagulation rate of patients whose CHA2DS2-VASc score ≥ 2 was 50.4%. Significant differences were observed in the anticoagulation rate amongst different admission years, admission departments, age groups, combined diseases and bleeding risk groups (all P < 0.05). A CRT decision tree model was constructed to analyse the influencing factors of anticoagulation in county-level hospitals. Finally, 15 variables including main diagnosis of atrial fibrillation, coronary heart disease, heart failure, number of comorbid diseases, department of admission, risk of stroke and bleeding, CHA2DS2-VASc score were included. The accuracy of the model was 65.0%, and the area under the ROC curve was 0.70. Conclusion The anticoagulation rate of patients with atrial fibrillation in county hospitals in eastern China has improved to a certain extent, but there is still room for improvement compared with tertiary hospitals. In addition, the anticoagulation standardization of doctors in county-level hospitals needs to be improved, and the training of doctors in county-level hospitals in anticoagulation treatment of atrial fibrillation still needs to be strengthened in the future. -
Key words:
- County hospital /
- Atrial fibrillation /
- Anticoagulation /
- Current situation /
- Influencing factors
-
表 1 2018—2019年3家县级医院房颤患者基本情况
项目 类别 例(%) 性别 男性 1 291(52.65) 女性 1 161(47.35) 职业转换 非农民 628(25.61) 农民 1 824(74.39) 入院年份 2018年 1 027(41.88) 2019年 1 425(58.12) 抗栓情况 未抗栓 482(19.66) 抗栓 1 970(80.34) 仅抗血小板 745(30.38) 仅抗凝 559(22.80) 抗凝联合抗血小板 666(27.16) 抗凝情况 未抗凝 1 227(50.04) 抗凝 1 225(49.96) 注射抗凝药 449(18.31) 口服抗凝药 1 013(41.31) 华法林 896(36.54) 利伐沙班 139(5.67) 达比加群 5(0.20) 合计 2 452(100.00)  下载: 导出CSV
下载: 导出CSV
表 2 2018—2019年3家县级医院房不同卒中风险分组抗凝情况
组别 整体 未抗凝 抗凝 例数 占比(%) 例数 占比(%) 例数 占比(%) CHA2DS2-VASc≥2分 2 081 84.87 1 032 49.59 1 049 50.41 CHA2DS2-VASc<2分 371 15.13 195 52.56 176 47.44
下载: 导出CSV
表 3 2018—2019年3家县级医院房颤患者抗凝治疗基本情况差异性分析[例(%)]
组别 例数 未抗凝 抗凝 χ2值 P值 年龄 38.101 <0.001 60岁及以下 291 121(41.6) 170(58.4) 61~70岁 607 258(42.5) 349(57.5) 71~80岁 692 360(52.0) 332(48.0) 80岁以上 862 488(56.6) 374(43.4) 性别 1.467 0.226 男性 1 291 661(51.2) 630(48.8) 女性 1 161 566(48.8) 595(51.2) 职业 0.988 0.320 农民 1 824 902(49.5) 922(50.5) 非农民 628 325(51.8) 303(48.2) 入院年份 6.064 0.014 2018年 1 027 544(53.0) 483(47.0) 2019年 1 452 683(47.9) 742(52.1)
下载: 导出CSV
表 4 2018—2019年3家县级医院房颤患者临床特征差异性分析[例(%)]
组别 例数 未抗凝 抗凝 χ2值 P值 是否房颤主诊断 178.719 <0.001 房颤非主诊断 2 049 1 148(56.0) 901(44.0) 房颤为主诊断 403 79(19.6) 324(80.4) 入院科室 145.456 <0.001 ICU 131 85(64.9) 46(35.1) 急诊 56 20(35.7) 36(64.3) 介入 54 19(35.2) 35(64.8) 内科 1 953 891(45.6) 1 062(54.4) 外科 185 148(80.0) 37(20.0) 五官 32 30(93.8) 2(6.2) 中医康复 41 34(82.9) 7(17.1) 合并疾病 冠心病 1 061 442(41.7) 619(58.3) 52.561 <0.001 未合并冠心病 1 391 783(56.3) 608(43.7) 糖尿病 107 107(50.0) 214(100.0) < 0.001 0.990 未合并糖尿病 2 238 1 118(50.0) 1 120(50.0) 高血压 1 003 519(51.7) 484(48.3) 1.971 0.160 未合并高血压 1 449 706(48.7) 743(51.3) 心力衰竭 1 087 423(38.9) 664(61.1) 96.690 <0.001 未合并心力衰竭 1 365 802(58.8) 563(41.2) ACS 98 37(37.8) 61(62.2) 6.163 0.013 未合并ACS 2 354 1 188(50.5) 1 166(49.5) 缺血性卒中 470 242(51.5) 228(48.5) 0.488 0.485 未合并缺血性卒中 1 982 983(49.6) 999(50.4) 心功能不全 1 080 484(44.8) 596(55.2) 21.086 <0.001 未合并心功能不全 1 372 741(54.0) 631(46.0) COPD 109 71(65.1) 38(34.9) 10.399 0.001 未合并COPD 2 343 1 154(49.3) 1 189(50.7) 出血性卒中 29 22(75.9) 7(24.1) 7.827 0.005 未合并出血性卒中 2 423 1 203(49.6) 1 220(50.4) 慢性缺血性心脏病 56 13(23.2) 43(76.8) 16.497 <0.001 未合并慢性缺血性心脏病 2 396 1 212(50.6) 1 184(49.4) 外周动脉疾病 90 65(72.2) 25(27.8) 18.388 <0.001 未合并外传动脉疾病 2 362 1 160(49.1) 1 202(50.9) 高脂血症 31 15(48.4) 16(51.6) 0.034 0.853 未合并高脂血症 2 421 1 210(50.0) 1 211(50.0)
下载: 导出CSV
表 5 2018—2019年3家县级医院房颤患者卒中及出血风险差异性分析[例(%)]
组别 例数 未抗凝 抗凝 χ2值 P值 卒中风险评分 1.110 0.292 CHA2DS2-VASc<2分 371 195(52.6) 176(47.4) CHA2DS2-VASc≥2分 2 081 1 032(49.6) 1 049(50.4) 出血风险评分 16.853 <0.001 HAS-BLED<3分 1 352 626(46.3) 726(53.7) HAS-BLED≥3 1 100 601(54.6) 499(45.4)
下载: 导出CSV
表 6 县级医院卒中高风险房颤患者抗凝治疗影响因素及其重要性
序号 纳入变量 变量重要性 1 房颤主要诊断 0.26 2 冠心病 0.24 3 心力衰竭 0.17 4 合并疾病数量 0.09 5 入院科别 0.06 6 慢性缺血性心脏病 0.04 7 心功能不全 0.04 8 ACS 0.03 9 CHA2DS2-VASc评分 0.02 10 HAS-BLED高风险(分数≥3分) 0.02 11 年龄分组 0.02 12 入院年份 0.01 13 高血压 0.01 14 缺血性卒中 4.68×10-6 15 高脂血症 2.11×10-6
下载: 导出CSV
-
[1] 黄从新. 中国心房颤动防治现状蓝皮书[M]. 北京: 人民卫生出版社, 2019: 15. [2] 赵锦星, 杨晓东. 阿司匹林联合氯吡格雷与华法林进行心房颤动抗凝治疗的安全性对比[J]. 中国现代药物应用, 2020, 14(19): 150-152. https://www.cnki.com.cn/Article/CJFDTOTAL-ZWYY202019069.htm [3] 邹文孝, 邹文淑, 王译, 等. 心房颤动患者的脑卒中预防性治疗[J]. 中华老年心脑血管病杂志, 2017, 19(9): 1007-1008. doi: 10.3969/j.issn.1009-0126.2017.09.030 [4] 黄从新, 张澍, 黄德嘉, 等. 心房颤动: 目前的认识和治疗的建议-2018[J]. 中国心脏起搏与心电生理杂志, 2018, 32(4): 315-368. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGXZ201804002.htm [5] LACOSTE J L, HANSEN C L. Antithrombotic therapy in patients with atrial fibrillation undergoing coronary artery stenting[J]. Am J Health Syst Pharm, 2019, 76(18): 1395-1402. doi: 10.1093/ajhp/zxz152 [6] KIRCHHOF P, BENUSSI S, KOTECHA D, et al. 2016 ESC Guidelines for the management of atrialfibrillation developed in collaboration with EACTS[J]. Eur Heart J, 2016, 37(38): 2893-2962. doi: 10.1093/eurheartj/ehw210 [7] 董霞, 张华, 王维平, 等. 老年房颤患者华法林抗凝治疗不足现状及原因[J]. 医学研究与教育, 2016, 33(2): 40-46. doi: 10.3969/j.issn.1674-490X.2016.02.009 [8] 周俊, 李志明, 李双, 等. 上海市社区老年人群心房颤动的流行病学调查[J]. 南京医科大学学报: 自然科学版, 2018, 38(9): 1314-1318. https://www.cnki.com.cn/Article/CJFDTOTAL-NJYK201809030.htm [9] 李欣彦, 汤颖, 孙红伟, 等. 合并阵发性心房颤动的急性缺血性脑卒中患者临床特征及预后研究[J]. 中华全科医学, 2019, 17(8): 1403-1407. https://www.cnki.com.cn/Article/CJFDTOTAL-SYQY201908044.htm [10] 朱静, 徐健, 苏浩, 等. 左心耳封堵治疗非瓣膜性房颤的安全性和有效性[J]. 中华全科医学, 2020, 18(8): 1261-1264. https://www.cnki.com.cn/Article/CJFDTOTAL-SYQY202008005.htm [11] 赵翠, 朱俊, 刘明名, 等. 不同级别医院心房颤动/心房扑动急诊处理用药分析[J]. 临床心血管病杂志, 2021, 37(2): 167-171. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202102016.htm [12] 孙卫红, 王晨希, 万桂兵, 等. 基层二甲医院单中心连续3年非瓣膜性心房颤动住院患者抗凝现状分析[J]. 中国心脏起搏与心电生理杂志, 2020, 34(6): 540-544. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGXZ202006007.htm [13] CHIANG C E, OKUMURA K, ZHANG S, et al. 2017 consensus of the Asia Pacific Heart Rhythm Society on stroke prevention in atrial fibrillation[J]. J Arrhythm, 2017, 33(4): 345-367. doi: 10.1016/j.joa.2017.05.004 [14] ETERSON E D, ASHTON V, CHEN Y W, et al. Comparative effectiveness, safety, and costs of rivaroxaban and warfarin among morbidly obese patients with atrial fibrillation[J]. Am Heart J, 2019, 212: 113-119. doi: 10.1016/j.ahj.2019.02.001 [15] 胡耀武. 不同华法林抗凝强度对高龄冠心病伴非瓣膜性房颤患者疗效及安全性的影响[J]. 临床合理用药杂志, 2021, 14(4): 50-51. https://www.cnki.com.cn/Article/CJFDTOTAL-PLHY202104018.htm [16] 闫静静, 秦明照. 亚洲心房颤动抗凝现状及与非亚洲抗凝策略的比较[J]. 心血管病学进展, 2018, 39(6): 884-888. https://www.cnki.com.cn/Article/CJFDTOTAL-XXGB201806004.htm -

 点击查看大图
点击查看大图
图(1) / 表(6)
计量
- 文章访问数: 99
- HTML全文浏览量: 114
- PDF下载量: 5
- 被引次数: 0
