

Prognostic value of apolipoprotein A1 in elderly patients with ischemic cardiomyopathy and heart failure
-
摘要:
目的 观察老年缺血性心肌病心衰患者血清载脂蛋白A1(apoA1)水平,探究血清apoA1对老年缺血性心肌病心衰患者预后的价值。 方法 选取2018年3月—2019年12月符合入组标准的在南京鼓楼医院心血管内科住院的老年缺血性心肌病心衰患者,电话随访终点事件。根据是否发生心源性死亡将患者分为2组,比较不同亚组住院期间的基线资料(年龄、性别、BMI等)、血清学指标(BNP、apoA1、HDL-C等)和影像学指标(超声心动图)。 结果 共纳入105例患者,其中9例(8.7%)在随访期间发生心源性死亡。比较2组数据的年龄、性别、血压、心率、BMI、吸烟饮酒史、合并症、用药等方面,发现纽约心功能等级高、合并地高辛用药史患者病死率升高(P < 0.05),余差异均无统计学意义。使用单因素分析初步筛查可能的影响预后的因素,发现在发生心源性死亡组中,BNP、球蛋白升高,HDL-C及apoA1降低(P < 0.05);多因素logistic分析提示apoA1是发生心源性死亡的独立危险因素(OR<0.001,P=0.007)。将患者按照apoA1水平分为低值组和高值组,发现低值组具有更高的CRP水平(t=3.505,P < 0.01);将球蛋白、HDL-C、apoA1、BNP联合绘制ROC曲线,ROC曲线下面积为0.863,提示模型预测效果较好。 结论 ApoA1为老年缺血性心肌病心衰患者发生心源性死亡的独立危险因素,能较好地预测预后。 Abstract:Objective To observe the level of serum apolipoprotein A1 (apoA1) in elderly patients with ischemic cardiomyopathy and heart failure, and to explore the prognostic value of serum apoA1 in elderly patients with ischemic cardiomyopathy and heart failure. Methods Elderly patients with ischemic cardiomyopathy and heart failure hospitalized in the Cardiology Department of Nanjing Drum Tower Hospital from March 2018 to December 2019 were selected retrospectively. The end events were followed up by telephone. The patients were divided into two groups according to whether cardiac death occurred or not. The baseline data (age, gender, BMI, etc.), serological indexes (BNP, apoA1, HDL-C, etc.) and imaging indexes (echocardiography) of different subgroups were compared. Results A total of 105 patients were included, of which 9 cases (8.7%) had cardiac death during follow-up. The age, gender, blood pressure, heart rate, BMI, smoking and drinking history, complications and medication history were compared between the two groups. It was found that the mortality rate of patients with higher the New York Heart Association (NYHA) grade and digoxin medication history increased (P < 0.05), but there was no significant difference in the rest between the two groups. Univariate analysis showed that the increase of BNP and globulin and the decrease of HDL-C and apoA1 were possible prognostic factors in the group of cardiac death (P < 0.05). Multivariate logistic regression analysis showed that apoA1 was an independent risk factor for cardiac death (OR < 0.001, P=0.007). The patients were divided into low value group and high value group according to the level of apoA1. It was found that the low value group had a higher level of C-reactive protein (t=3.505, P < 0.01). The ROC curve of globulin, HDL cholesterol, apoA1, BNP was drawn together, and area under ROC curve was 0.863, indicating the preferable prediction effect of the model. Conclusion ApoA1 is an independent risk factor for cardiac death in elderly patients with ischemic cardiomyopathy and heart failure. -
Key words:
- Apolipoprotein A1 /
- Ischemic cardiomyopathy /
- Heart failure
-

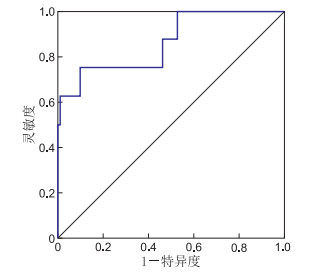
图 1 多因素联合预测老年缺血性心肌病心衰患者心源性死亡ROC曲线
Figure 1. ROC curve of multiple factors combined to predict cardiac death in elderly patients with ischemic cardiomyopathy and heart failure
表 1 心源性死亡组与未发生心源性死亡组缺血性心肌病患者临床基本资料比较
Table 1. Comparison of basic clinical data of patients with ischemic cardiomyopathy between cardiac death group and non-cardiac death group
项目 无心源性死亡
(n=96)心源性死亡
(n=9)统计量 P值 项目 无心源性死亡
(n=96)心源性死亡
(n=9)统计量 P值 年龄[M(P25, P75),岁] 75(69, 83) 84(71, 86) -1.312a 0.192 卒中[例(%)] 性别[例(%)] 1.538b 0.215 否 80(83.33) 8(88.89) < 0.001b 0.999 男性 73(76.04) 9(100.00) 是 16(16.67) 1(11.11) 女性 23(23.96) 0 心肌梗死[例(%)] BMI(x±s) 24.09±3.42 22.15±2.63 1.644c 0.103 否 46(47.92) 3(33.33) 0.498 心率[M(P25, P75),次/min] 77(64, 85) 79(67, 90) -0.878a 0.382 是 50(52.08) 6(66.67) 舒张压(x±s,mm Hg) 75.03±15.15 77.11±17.62 -0.384c 0.702 阿司匹林[例(%)] 收缩压(x±s,mm Hg) 130.09±20.68 123.11±16.67 0.974c 0.332 否 33(35.11) 5(55.56) 0.728b 0.394 NYHA分级[例(%)] 是 61(64.90) 4(44.44) Ⅰ 3(3.13) 0 9.211b 0.019 呋塞米[例(%)] Ⅱ 30(31.25) 0 否 23(24.47) 0 0.202d Ⅲ 38(39.58) 2(22.22) 是 71(75.53) 9(100.00) Ⅳ 25(26.04) 7(77.78) 地高辛[例(%)] 饮酒[例(%)] 否 86(91.49) 5(55.56) 7.108b 0.008 否 85(88.54) 8(88.89) < 0.001b 0.999 是 8(8.51) 4(44.44) 是 11(11.46) 1(11.11) SGLT2i[例(%)] 吸烟[例(%)] 否 92(97.87) 9(100.00) 0.999d 否 63(65.63) 7(77.78) 0.137b 0.712 是 2(2.13) 0 是 33(34.38) 2(22.22) 诺欣妥[例(%)] 糖尿病[例(%)] 否 71(75.53) 7(77.78) < 0.001b 0.999 否 56(58.33) 2(22.22) 3.002b 0.083 是 23(24.47) 2(22.22) 是 40(41.67) 7(77.78) 螺内酯[例(%)] 高血压病[例(%)] 否 20(21.28) 1(11.11) 0.084b 0.772 否 25(26.04) 3(33.33) 0.006b 0.937 是 74(78.72) 8(88.89) 是 71(73.96) 6(66.67) β受体阻滞剂[例(%)] COPD[例(%)] 否 15(15.96) 3(33.33) 0.726b 0.394 否 86(89.58) 9(100.00) 0.596d 是 79(84.04) 6(66.67) 是 10(10.42) 0 ACEI/ARB[例(%)] 房颤[例(%)] 否 42(44.68) 6(66.67) 0.834b 0.298 否 70(72.92) 5(55.56) 0.513b 0.474 是 52(55.32) 3(33.33) 是 26(27.08) 4(44.44) 甲亢[例(%)] 否 96(100.00) 9(100.00) 0.999d 是 0 0 注:a为Z值,b为χ2值,c为t值,d为采用Fisher精确经验。1 mm Hg=0.133 kPa。  下载: 导出CSV
下载: 导出CSV
表 2 心源性死亡组与未发生心源性死亡组缺血性心肌病患者实验室指标比较(x±s)
Table 2. Comparison of laboratory indexes in patients with ischemic cardiomyopathy in cardiac death group and non-cardiac death group
组别 例数 球蛋白(g/L) apoA1(g/L) HDL-C(mmol/L) BNP(pg/mL) 无心源性死亡 96 25.38±4.58 0.86±0.20 0.95±0.28 678.18±594.05 心源性死亡 9 29.64±6.58 0.63±0.12 0.74±0.32 1 352.63±1 036.87 统计量 -2.535 3.254 2.057 -2.833 P值 0.013 0.002 0.042 0.006
下载: 导出CSV
表 3 影响心源性死亡的多因素logistic回归分析
Table 3. Multivariate logistic regression analysis of cardiac death
项目 B SE Waldχ2 P值 OR值 95% CI 球蛋白 0.138 0.102 1.823 0.177 1.148 0.940~1.401 apoA1 -9.758 3.590 7.386 0.007 <0.001 0~0.066 LDL-C -0.402 0.592 0.460 0.498 0.669 0.210~2.137 HDL-C 1.774 1.994 0.791 0.374 5.892 0.118~293.483 BNP 0.001 <0.001 2.873 0.090 1.001 1.000~1.002 EF -0.039 0.109 0.125 0.723 0.962 0.777~1.191 吸烟 -0.204 1.126 0.033 0.856 0.815 0.090~7.410
下载: 导出CSV
表 4 apoA1高低水平分组后实验室指标的差异比较
Table 4. Comparison of differences in laboratory indicators after grouping high and low levels of apoA1
项目 低值组(n=49) 高值组(n=53) 统计量 P值 LAD(x±s, mm) 4.86±0.50 4.64±0.60 1.990a 0.049 C反应蛋白[M(P25, P75), mg/L] 13.65(5.40, 40.45) 3.25(2.42, 5.00) -3.829b 0.001 中性粒细胞百分率[M(P25, P75), %] 68.35(56.25, 71.65) 63.85(52.90, 69.53) -2.117b 0.034 淋巴细胞百分率[M(P25, P75), %] 20.10(17.20, 29.20) 25.75(18.53, 34.35) -2.361b 0.018 尿酸[M(P25, P75), μmol/L] 454.00(374.25, 561.25) 362.50(296.00, 438.50) -2.170b 0.030 直接胆红[M(P25, P75), μmol/L] 3.95(2.70, 5.83) 2.65(2.03, 3.08) -2.312b 0.021 白蛋白[M(P25, P75), g/L] 36.65(34.98, 39.98) 38.35(37.28, 40.08) -2.746b 0.006 游离甲状腺(x±s, pmol/L) 18.34±3.02 16.81±3.46 2.177a 0.032 注:a为t值,b为Z值。
下载: 导出CSV
-
[1] TOMASONI D, ADAMO M, LOMBARDI C M, et al. Highlights in heart failure[J]. ESC Heart Fail, 2019, 6(6): 1105-1127. doi: 10.1002/ehf2.12555 [2] KATZ D, GAVIN M C. Stable ischemic heart disease[J]. Ann Intern Med, 2019, 171(3): ITC17-ITC32. doi: 10.7326/AITC201908060 [3] COCHRAN B J, ONG K L, MANANDHAR B, et al. APOA1: A protein with multiple therapeutic functions[J]. Curr Atheroscler Rep, 2021, 23(3): 11. doi: 10.1007/s11883-021-00906-7 [4] TONRY C, MCDONALD K, LEDWIDGE M, et al. Multiplexed measurement of candidate blood protein biomarkers of heart failure[J]. ESC Heart Fail, 2021, 8(3): 2248-2258. doi: 10.1002/ehf2.13320 [5] 王丽君, 郜珊珊. 血清apoA1水平与冠心病患者左室收缩功能的关系[J]. 临床心血管病杂志, 2021, 37(11): 988-991. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202111004.htmWANG L J, GAO S S. Relationship between serum apoA1 levels and left ventricular systolic function in patients with coronary artery disease[J]. Journal of Clinical Cardiology, 2021, 37(11): 988-991. https://www.cnki.com.cn/Article/CJFDTOTAL-LCXB202111004.htm [6] 韩智红, 吴学思. 缺血性左心室收缩功能障碍-心血管病医生的挑战[J]. 心肺血管病杂志, 2018, 37(5): 381-383. doi: 10.3969/j.issn.1007-5062.2018.05.001HAN Z H, WU X S. Ischemic left ventricular systolic dysfunction with-cardiologist challenges[J]. Journal of Cardiovascular and Pulmonary Diseases, 2018, 37(5): 381-383. doi: 10.3969/j.issn.1007-5062.2018.05.001 [7] ELGENDY I Y, MAHTTA D, PEPINE C J, et al. Medical therapy for heart failure caused by ischemic heart disease[J]. Circ Res, 2019, 124(11): 1520-1535. doi: 10.1161/CIRCRESAHA.118.313568 [8] 茅焕豪, 叶剑飞, 郑伟峰, 等. 左西孟旦联合冻干重组人脑利钠肽对缺血性心肌病患者心室重构改善作用的研究[J]. 中华全科医学, 2021, 19(11): 1861-1863, 1950. doi: 10.16766/j.cnki.issn.1674-4152.002186MAO H H, YE J F, ZHENG W F, et al. Effect of levosimendan combined with lyophilised recombinant human brain natriuretic peptide on ventricular remodelling in patients with ischemic cardiomyopathy[J]. Chinese Journal of General Practice, 2021, 19(11): 1861-1863, 1950. doi: 10.16766/j.cnki.issn.1674-4152.002186 [9] 何新为, 陈加仕, 郭勤生. 左室射血功能与NT-proBNP对缺血性心肌病预后的预测价值研究[J]. 中国处方药, 2020, 18(2): 162-163. doi: 10.3969/j.issn.1671-945X.2020.02.093HE X W, CHEN J S, GUO Q S. Prognostic value of left ventricular ejection function and NT-proBNP in patients with ischemic cardiomyopathy[J]. Journal Of China Prescription Drug, 2020, 18(2): 162-163. doi: 10.3969/j.issn.1671-945X.2020.02.093 [10] 冯婷婷, 贾淑杰, 赵全明. 高密度脂蛋白胆固醇水平与慢性心力衰竭严重程度的相关性[J]. 心肺血管病杂志, 2018, 37(8): 735-739. doi: 10.3969/j.issn.1007-5062.2018.08.007FENG T T, JIA S J, ZHAO Q M. Correlationship between high density lipoprotein cholesterol levels and NYHA classification of chronic heart failure in patients[J]. Journal of Cardiovascular and Pulmonary Diseases, 2018, 37(8): 735-739. doi: 10.3969/j.issn.1007-5062.2018.08.007 [11] DEGORICIJA V, POTOCNJAK I, GASTRAGER M, et al. HDL subclasses and mortality in acute heart failure patients[J]. Clin Chim Acta, 2019, 490: 81-87. doi: 10.1016/j.cca.2018.12.020 [12] SPOSITO A C, CARMO H R, BARRETO J, et al. HDL-targeted therapies during myocardial infarction[J]. Cardiovasc Drugs Ther, 2019, 33(3): 371-381. doi: 10.1007/s10557-019-06865-1 [13] ZANONI P, VON ECKARDSTEIN A. Inborn errors of apolipoprotein A-I metabolism: Implications for disease, research and development[J]. Curr Opin Lipidol, 2020, 31(2): 62-70. doi: 10.1097/MOL.0000000000000667 [14] RICHART A L, REDDY M, KHALAJI M, et al. Apo AI nanoparticles delivered post myocardial infarction moderate inflammation[J]. Circ Res, 2020, 127(11): 1422-1436. doi: 10.1161/CIRCRESAHA.120.316848 [15] ADAMO L, ROCHA-RESENDE C, PRABHU S D, et al. Reappraising the role of inflammation in heart failure[J]. Nat Rev Cardiol, 2020, 17(5): 269-285. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 352
- HTML全文浏览量: 155
- PDF下载量: 21
- 被引次数: 0
