

Safety and efficacy of intravenous tirofiban after endovascular treatment of acute cerebral infarction
-
摘要:
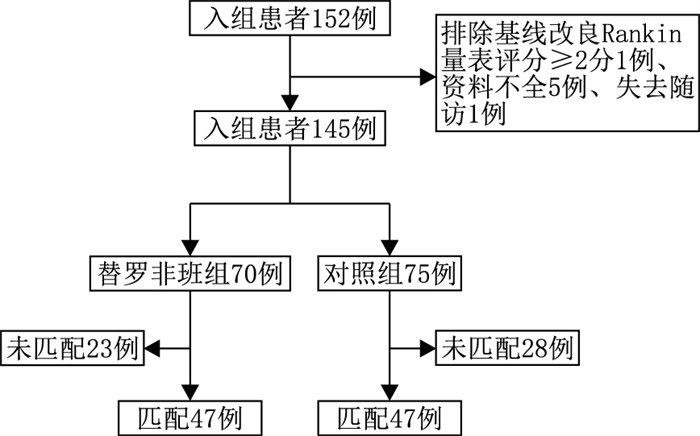
目的 探讨急性脑梗死血管内治疗后静脉注射替罗非班的安全性和有效性。 方法 回顾性纳入2019年9月—2021年3月陆军军医大学大坪医院神经内科收治的急性脑梗死并行血管内治疗患者152例。根据血管内治疗后是否使用替罗非班静脉滴注将其分为替罗非班组和对照组。采用1∶ 1比例的倾向评分匹配分析平衡2组的基线资料。观察主要终点包括安全性和有效性。安全性为症状性颅内出血(sICH)、任何出血、90 d内复发和病死率;有效性为出院时美国国立卫生研究院卒中量表(NIHSS)评分及90 d预后良好率[改良Rankin量表(mRS)评分0~2分]。 结果 最终共纳入患者145例,其中替罗非班组70例,对照组75例,替罗非班组出院时NIHSS评分[4(2, 13) vs. 11(3, 16),P=0.002]明显优于对照组患者;替罗非班组与对照组sICH发生率[7(10.0%) vs. 12(16.0%), P=0.284]、90 d预后良好率、任何出血、复发和病死率差异均无统计学意义(均P>0.05)。经倾向性评分成功匹配47对,2组安全性及有效性指标比较差异无统计学意义(均P>0.05)。 结论 急性脑梗死血管内治疗后静脉注射替罗非班治疗是安全的。匹配前替罗非班可以改善急性脑梗死血管内治疗后患者的出院时NIHSS评分,但在90 d预后良好率上并无获益;匹配后,替罗非班组患者在出院时及90 d的预后良好率均无获益。 Abstract:Objective To evaluate the safety and efficacy of intravenous tirofiban after endovascular treatment for patients with acute cerebral infarction. Methods A total of 152 patients with acute cerebral infarction undergoing endovascular treatment in the Department of Neurology of Daping Hospital, Army Military Medical University from September 2019 to March 2021 were retrospectively included. They were divided into the tirofiban group and control group according to whether tirofiban was injected intravenously after endovascular treatment. The baseline of the two groups was balanced by 1∶ 1 propensity score matching analysis. The main end points included safety and effectiveness. The safety was symptomatic intracranial haemorrhage (sICH), any haemorrhage, recurrence within 90 days and mortality. The effectiveness was National Institutes of Health Stroke Scale (NIHSS) score at discharge and 90-day good prognosis rate (modified Rankin score: 0-2). Results A total of 145 patients were included, including 70 in the tirofiban group and 75 in the control group. The NIHSS score of the tirofiban group at discharge [4(2, 13) vs. 11(3, 16), P=0.002] was significantly better than that of the control group. Moreover, there was no significant difference in the incidence of sICH [7(10.0%) vs. 12(16.0%), P=0.284] 90-day prognosis, any bleeding, recurrence and mortality (all P>0.05). Forty-seven pairs were successfully matched by propensity score. There was no significant difference in safety and effectiveness between the two groups (all P>0.05). Conclusion Intravenous tirofiban is safe after endovascular treatment of acute cerebral infarction. Pre-matching tirofiban can improve the NIHSS score at discharge of patients with acute cerebral infarction after endovascular treatment, but it has no benefit in the 90-day prognosis rate. After matching, there was no benefit in the good prognosis of tirofiban patients at discharge and 90 days. -

图 1 急性脑梗死血管内治疗患者倾向性评分匹配流程图
Figure 1. Flow chart of propensity score matching in patients with acute cerebral infarction treated with endovascular therapy
表 1 2组急性大血管闭塞经血管内治疗患者倾向性评分匹配前临床特征比较
Table 1. Comparison of clinical characteristics before propensity score matching between two groups of patients with acute macrovascular occlusion treated by endovascular therapy
组别 例数 年龄[M(P25, P75), 岁] 性别(男/女,例) 心血管危险因素[例(%)] TOAST分型[例(%)] 高血压 冠心病 吸烟 大动脉粥样硬化型 心源性栓塞 其他 替罗非班组 70 64(54,72) 48/22 45(64.3) 14(20.0) 15(21.4) 35(50.0) 30(47.1) 5(7.1) 对照组 75 71(60,78) 36/39 46(61.3) 30(40.0) 14(18.7) 34(45.3) 38(50.7) 3(4.0) 统计量 -2.733a 6.287b 0.135b 6.852b 4.970b 0.316b 0.887b P值 0.006 0.012 0.713 0.009 0.026 0.574 0.346 0.483c 组别 例数 基线NIHSS评分[M(P25, P75), 分] 静脉溶栓[例(%)] 入院收缩压(x±s, mm Hg) 发病到入院时间[M(P25, P75), 分] 穿刺到再通时间[M(P25, P75), 分] 血管再通[mTICI≥2b,例(%)] 替罗非班 70 11(5,19) 26(37.1) 150.40±25.81 364(183,563) 155(108,198) 59(84.3) 对照组 75 16(11,21) 42(56.0) 147.07±25.27 250(130,351) 115(83,182) 62(82.7) 统计量 -3.059a 5.170b 0.157d -2.315a -2.163a 0.069b P值 0.002 0.023 0.433 0.021 0.031 0.793 注:a为Z值,b为χ2值,c为采用Fisher精确检验, d为t值;1 mm Hg=0.133 kPa。  下载: 导出CSV
下载: 导出CSV
表 2 2组急性大血管闭塞经血管内治疗患者倾向性评分匹配前安全性和有效性指标比较
Table 2. Comparison of safety and efficacy indicators before propensity score matching between two groups of patients with acute macrovascular occlusion treated with endovascular therapy
组别 例数 安全性指标 有效性指标 任何出血[例(%)] sICH[例(%)] 90 d复发[例(%)] 90 d死亡[例(%)] 出院时NIHSS评分[M(P25, P75), 分] 90 d mRS 0~2分[例(%)] 替罗非班组 70 14(20.0) 7(10.0) 2(2.9) 3(4.3) 4(2,13) 57(81.4) 对照组 75 24(32.0) 12(16.0) 0 8(10.7) 11(3,16) 51(68.0) 统计量 2.696a 1.144a 2.103a -3.047c 3.435a P值 0.101 0.284 0.497b 0.147 0.002 0.064 注:a为χ2值, b为采用Fisher精确检验, c为Z值。
下载: 导出CSV
表 3 2组急性大血管闭塞经血管内治疗患者倾向性评分匹配后临床特征比较
Table 3. Comparison of clinical characteristics between two groups of patients with acute macrovascular occlusion treated by endovascular propensity score matching
组别 例数 年龄[M(P25, P75), 岁] 性别(男/女,例) 心血管危险因素[例(%)] TOAST分型[例(%)] 高血压 冠心病 吸烟 大动脉粥样硬化型 心源性栓塞型 其他 替罗非班组 47 67(53,74) 31/16 30(63.8) 11(23.4) 19(40.4) 30(63.8) 15(31.9) 2(4.3) 对照组 47 66(54,76) 29/18 26(55.3) 14(29.8) 16(34.0) 36(76.6) 10(21.3) 1(2.1) 统计量 -0.174a 0.184b 0.707b 0.490b 0.410b 1.831b 1.362b P值 0.862 0.668 0.401 0.484 0.522 0.176 0.243 0.999c 组别 例数 基线NIHSS评分[M(P25, P75), 分] 静脉溶栓[例(%)] 入院收缩压(x±s, mm Hg) 发病到入院时间[M(P25, P75), 分] 穿刺到再通时间[M(P25, P75), 分] 血管再通(mTICI≥2b) [例(%)] 替罗非班组 47 14(6,20) 18(38.3) 151.38±25.80 369(180,570) 160(110,210) 40(85.1) 对照组 47 13(9,18) 27(54.4) 141.15±25.30 270(172,394) 120(85,210) 38(80.9) 统计量 -0.155a 3.453b -1.388d -1.187a -1.161a 0.301b P值 0.877 0.063 0.168 0.235 0.246 0.583 注:a为Z值,b为χ2值,c为采用Fisher精确检验, d为t值。
下载: 导出CSV
表 4 2组急性大血管闭塞经血管内治疗患者倾向性评分匹配后安全性和有效性指标比较
Table 4. Comparison of safety and efficacy indexes between two groups of patients with acute macrovascular occlusion treated by endovascular treatment after propensity score matching
组别 例数 安全性指标 有效性指标 任何出血[例(%)] sICH[例(%)] 90 d复发[例(%)] 90 d死亡[例(%)] 出院时NIHSS评分[M(P25, P75), 分] 90 d mRS 0~2分[例(%)] 替罗非班组 70 11(23.4) 4(8.5) 0 3(6.4) 4(2, 15) 35(74.5) 对照组 75 16(34.0) 8(17.0) 1(2.1) 3(6.4) 10(3, 14) 36(76.6) 统计量 1.299a 1.528a -0.885c 0.058a P值 0.254 0.216 0.999b 0.999b 0.376 0.810 注:a为χ2值, b为采用Fisher精确检验, c为Z值。
下载: 导出CSV
-
[1] WANG W Z, JIANG B, SUN H X, et al. Prevalence, incidence, and mortality of stroke in China: Results from a nationwide population-based survey of 480 687 adults[J]. Circulation, 2017, 135(8): 759771. [2] BENJAMIN E J, VIRANI S S, CALLAWAY C W, et al. Heart disease and stroke statistics-2018 update: A report from the American Heart Association[J]. Circulation, 2018, 137(12): e67-e492. [3] BERKHEMER O A, FRANSEN P S, BEUMER D, et al. A randomized trial of intraarterial treatment for acute ischemic stroke[J]. N Engl J Med, 2015, 372(1): 11-20. doi: 10.1056/NEJMoa1411587 [4] BRACARD S, DUCROCQ X, MAS J L, et al. Mechanical thrombectomy after intravenous alteplase versus alteplase alone after stroke (THRACE): A randomised controlled trial[J]. Lancet Neurol, 2016, 15(11): 1138-1147. doi: 10.1016/S1474-4422(16)30177-6 [5] JOVIN T G, CHAMORRO A, COBO E, et al. Thrombectomy within 8 hours after symptom onset in ischemic stroke[J]. N Engl J Med, 2015, 372(24): 2296-2306. doi: 10.1056/NEJMoa1503780 [6] MARTO J P, STROMBO D, HAJDU S D, et al. Twenty-four-hour reocclusion after successful mechanical thrombectomy: Associated factors and long-term prognosis[J]. Stroke, 2019, 50(10): 2960-2963. doi: 10.1161/STROKEAHA.119.026228 [7] LI W, LIN L, ZHANG M, et al. Safety and preliminary efficacy of early tirofiban treatment after alteplase in acute ischemic stroke patients[J]. Stroke, 2016, 47(10): 2649-2651. doi: 10.1161/STROKEAHA.116.014413 [8] ZHAO W B, CHE R W, SHANG S Y, et al. Low-dose tirofiban improves functional outcome in acute ischemic stroke patients treated with endovascular thrombectomy[J]. Stroke, 2017, 48(12): 3289-3294. doi: 10.1161/STROKEAHA.117.019193 [9] PAN X, ZHENG D, ZHENG Y, et al. Safety and efficacy of tirofiban combined with endovascular treatment in acute ischemic[J]. Stroke, 2019, 26(8): 1105-1110. [10] 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国急性缺血性脑卒中诊治指南2018[J]. 中华神经科杂志, 2018, 51(9): 666-682. doi: 10.3760/cma.j.issn.1006-7876.2018.09.004Neurology branch of Chinese Medical Association, cerebrovascular disease group of Neurology branch of Chinese Medical Association, Chinese guidelines for the diagnosis and treatment of acute ischemic stroke 2018[J]. Chinese Journal of Neurology, 2018, 51(9): 666-682. doi: 10.3760/cma.j.issn.1006-7876.2018.09.004 [11] 朱余友, 王黎, 刘天龙. 大脑中动脉M2段急性闭塞性机械取栓疗效分析[J]. 中华全科医学, 2021, 19(10): 1633-1649. doi: 10.16766/j.cnki.issn.1674-4152.002129ZHU Y Y, WANG L, LIU T L. Analysis of therapeutic effect of mechanical thrombectomy for acute occlusion of M2 segment of middle cerebral artery[J]. Chinese general practice, 2021, 19(10): 1633-1649. doi: 10.16766/j.cnki.issn.1674-4152.002129 [12] 蔡必扬, 郭洪权, 李华. 关于美国国立卫生研究院卒中量表翻译的警示[J]. 中华神经科杂志, 2017, 50(9): 712. doi: 10.3760/cma.j.issn.1006-7876.2017.09.020CAI B Y, GUO H Q, LI H. A warning on the translation of the National Institutes of Health Stroke Scale[J]. Chinese Journal of Neurology, 2017, 50(9): 712. doi: 10.3760/cma.j.issn.1006-7876.2017.09.020 [13] 郝佳妮, 屈洪党. 大动脉粥样硬化型脑梗死的诊断与治疗[J]. 中华全科医学, 2019, 17(1): 4-6. http://www.zhqkyx.net/article/id/2033738d-94df-4bf6-8635-7adbd74bad7eHAO J N, QU H D. Diagnosis and treatment of large atherosclerotic cerebral infarction[J]. Chinese general practice, 2019, 17(1): 4-6. http://www.zhqkyx.net/article/id/2033738d-94df-4bf6-8635-7adbd74bad7e [14] ZHU F, HOSSU G, SOUDANT M, et al. Effect of emergent carotid stenting during endovascular therapy for acute anterior circulation stroke patients with tandem occlusion: A multicenter, randomized, clinical trial (TITAN) protocol[J]. Int J Stroke, 2021, 16(3): 342-348. doi: 10.1177/1747493020929948 [15] VON KUMMER R, BRODERICK J P, Campbell B C, et al. The Heidelberg bleeding classification: Classification of bleeding events after ischemic stroke and reperfusion therapy[J]. Stroke, 2015, 46(10): 2981-2986. doi: 10.1161/STROKEAHA.115.010049 [16] YANG M, HUO X, GAO F, et al. Low-dose rescue tirofiban in mechanical thrombectomy for acute cerebral large-artery occlusion[J]. Eur J Neurol, 2020, 27(6): 1056-1061. doi: 10.1111/ene.14170 [17] KELLERT L, HAMETNER C, ROHDE S, et al. Endovascular stroke therapy: Tirofiban is associated with risk of fatal intracerebral hemorrhage and poor outcome[J]. Stroke, 2013, 44(5): 1453-1455. doi: 10.1161/STROKEAHA.111.000502 [18] ZHANG S, HAO Y G, TIAN X G, et al. Safety of intra-arterial tirofiban administration in ischemic stroke patients after unsuccessful mechanical thrombectomy[J]. J Vasc Interv Radiol, 2019, 30(2): 141-147. doi: 10.1016/j.jvir.2018.08.021 [19] SUN C, LI X, ZHAO Z, et al. Safety and efficacy of tirofiban combined with mechanical thrombectomy depend on ischemic stroke etiology[J]. Front Neurol, 2019, 10: 1100. doi: 10.3389/fneur.2019.01100 [20] WANG X G, ZHANG L Q, LIAO X L, et al. Thrombolysis implementation and monitoring of acute ischemic stroke in China (TIMS-China) investigators. unfavorable outcome of thrombolysis in chinese patients with cardioembolic stroke: A prospective cohort study[J]. CNS Neurosci Ther, 2015, 21: 657-661. doi: 10.1111/cns.12421 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 269
- HTML全文浏览量: 61
- PDF下载量: 3
- 被引次数: 0
