

Clinical effect analysis of curettage and fenestration decompression for treating odontogenic cyst of jaw
-
摘要:
目的 探讨刮治术和开窗减压术治疗牙源性颌骨囊肿的临床疗效,为临床工作中术式的合理选择提供参考依据。 方法 回顾性分析2016年1月—2018年12月湖州师范学院附属第一医院收治的牙源性颌骨囊肿患者180例,根据术式不同分为2组,刮治组100例行囊肿刮治术,开窗组80例行开窗减压术。比较2组患者术后第3、6个月囊腔面积缩小百分率,比较2组患者术后第6个月的临床有效率,比较开窗组不同类型囊肿的开窗效果,并比较2组患者术后出现感染、出血、麻木及复发情况。 结果 开窗组术后第3、6个月囊腔面积缩小百分率均高于刮治组,差异有统计学意义(均P < 0.001)。术后第6个月,开窗组有效率为82.50%(66/80),刮治组有效率为69.00%(69/100),差异有统计学意义(P < 0.05)。开窗组开窗末期有效率为91.25%(73/80),角化囊肿单房型的开窗效果优于多房型,差异有统计学意义(P < 0.05),不同类型牙源性颌骨囊肿间开窗效果差异无统计学意义(P>0.05)。刮治组术后感染发生率为2.00%(2/100),下唇麻木发生率为1.00%(1/100),复发率为1.00%(1/100),开窗组术后未出现并发症。 结论 刮治术与开窗减压术均为目前治疗牙源性颌骨囊肿的有效方法,刮治术适用于小型颌骨囊肿或囊肿未侵犯颌骨周围重要解剖结构;开窗术相比刮治术操作简单、创伤小、术后并发症更少, 且能有效缩小囊腔并促进颌骨囊肿周围骨质新生,尤其适用于大-中型颌骨囊肿或病灶致骨质吸收严重者,利于二期手术彻底刮治,以保存颌骨功能。 Abstract:Objective To evaluate the clinical effect of curettage and fenestration decompression in the treatment of odontogenic cyst of jaw and provide reference for rational selection of surgical techniques in clinical work. Methods A retrospective analysis of 180 patients with odontogenic cyst of jaw from January 2016 to December 2018 in the First Affiliated Hospital of Huzhou Normal University was carried out. Patients were divided into two groups according to different surgical methods, 100 cases underwent cyst curettage and 80 cases fenestration decompression. The percentages of cyst area reduction at 3 and 6 months, clinical effective rate at 6 months postoperatively were compared between the two groups. The clinical effective rate of different types of cysts in the fenestration group were compared. The rate of postoperative infection, bleeding, numbness and recurrence were compared between the two groups. Results The percentage of cyst cavity area reduction in the fenestration group at 3 and 6 months after operation were significantly higher than that in curettage group, and the differences were statistically significant (all P < 0.01). At 6 months after operation, the effective rate of fenestration group was 82.50% (66/80) while that of curettage group was 69.00% (69/100), and the difference was statistically significant (P < 0.05). The total effective rate of fenestration group was 91.25% (73/80), effective rate of keratinizing cyst was better than that of multilocular type (P < 0.05), and there was no significant difference in fenestration effect between different cyst types (P>0.05). In curettage group, the rate of postoperative infection was 2.00% (2/100), the rate of lower lip numbness was 1.00% (1/100) and the recurrence rate was 1.00% (1/100). There was no postoperative complication in the fenestration group. Conclusion Both curettage and fenestration decompression are effective methods for the treatment of odontogenic cyst of jaw. Curettage is more suitable for small jaw cysts or cysts that do not invade important anatomical structures around the jaw. Compared to curettage, fenestration decompression is simpler to operate, less traumatic, and has fewer complications. Fenestration decompression can effectively reduce the cyst cavity and promotes bone regeneration around jaw cysts, which is especially suitable for large-medium-sized cysts, and is conducive to complete curettage in stage Ⅱ surgery to preserve function. -
Key words:
- Odontogenic cyst of jaw /
- Cyst curettage /
- Fenestration decompression
-

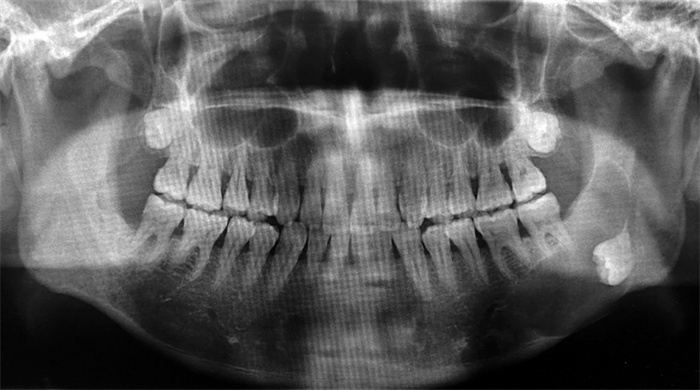
图 1 左下颌骨含牙囊肿术前全景片
Figure 1. Pre-operative panoramic X-ray of dental cyst of left mandible

图 2 左下颌骨含牙囊肿开窗减压术后12个月全景片
Figure 2. Panoramic X-ray at 12 months after fenestration decompression of dental cyst of left mandible
表 1 2组牙源性颌骨囊肿患者一般资料比较
Table 1. Comparison of the general data of the two groups of patients with odontogenic cyst
组别 例数 年龄(x±s,岁) 性别[例(%)] 囊肿直径(x±s,cm) 男性 女性 刮治组 100 37.89±10.74 57(57.0) 43(43.0) 3.46±1.12 开窗组 80 40.23±9.74 42(52.5) 38(47.5) 4.21±1.22 统计量 1.510a 0.364b 4.291a P值 0.133 0.546 < 0.005 注:a为t值,b为χ2值。  下载: 导出CSV
下载: 导出CSV
表 2 2组牙源性颌骨囊肿患者囊腔面积缩小率比较(x±s,%)
Table 2. Comparison of the percentages of cyst area reduction between curettage group and fenestration group(x±s, %)
组别 例数 术后3个月 术后6个月 刮治组 100 26.91±4.26 60.23±14.85 开窗组 80 31.14±5.03 70.00±13.39 t值 6.103 4.579 P值 < 0.001 < 0.001
下载: 导出CSV
表 3 2组牙源性颌骨囊肿患者临床有效率比较
Table 3. Comparison of clinical effective rate between curettage group and fenestration group
组别 例数 显效(例) 有效(例) 好转(例) 有效率(%) 刮治组 100 10 59 31 69.00 开窗组 80 8 58 14 82.50 注:2组有效率比较,χ2=4.320,P=0.038。
下载: 导出CSV
表 4 开窗组不同病理类型牙源性颌骨囊肿患者治疗效果
Table 4. Comparison of therapeutic effects of different pathological types in fenestration group
病理类型 例数 显效(例) 有效(例) 好转(例) 有效率(%) 根尖囊肿 15 8 6 1 93.33 含牙囊肿 19 7 11 1 94.74 角化囊肿 单房型 37 16 19 2 94.59 多房型 9 2 4 3 66.67 合计 80 33 40 7 91.25
下载: 导出CSV
-
[1] BILODEAU E A, COLLINS B M. Odontogenic cysts and neoplasms[J]. Surg Pathol Clin, 2017, 10(1): 177-222. doi: 10.1016/j.path.2016.10.006 [2] ZHANG L, PEI J, HUANG M, et al. Application of a new drainage plug for large mandibular cysts after fenestration decompression[J]. Ann Palliat Med, 2021, 10(1): 590-596. doi: 10.21037/apm-20-2464 [3] 徐芳, 郑刚. 大型颌骨囊肿开窗减压术联合囊肿塞治疗的临床应用[J]. 口腔颌面外科杂志, 2017, 27(3): 195-198. doi: 10.3969/j.issn.1005-4979.2017.03.009XU F, ZHENG G. Marsupialization with Space Obliteration in the Treatment of Large Cysts of the Jaws[J]. Journal of Oral and Maxillofacial Surgery, 2017, 27(3): 195-198. doi: 10.3969/j.issn.1005-4979.2017.03.009 [4] 苏屹坤, 王婧, 张桐菲, 等. 4 181例牙源性肿瘤及囊肿临床病理分析[J]. 中华口腔医学杂志, 2019, 54(8): 546-552. doi: 10.3760/cma.j.issn.1002-0098.2019.08.009SU Y K, WANG J, ZHANG T F, et al. Odontogenic tumors and odontogenic cysts: A clinical and pathological analysis of 4 181 cases[J]. Chinese Journal of Stomatology, 2019, 54(8): 546-552. doi: 10.3760/cma.j.issn.1002-0098.2019.08.009 [5] 王亮, 任镟伊, 应凯. 开窗术保留颌骨囊肿非病灶牙的临床分析[J]. 口腔颌面外科杂志, 2021, 31(3): 177-179. doi: 10.3969/j.issn.1005-4979.2021.03.009WANG L, REN X Y, YING K. Clinical analysis on preserving non-focused teeth of jaw cysts after fenestration management[J]. Journal of Oral and Maxillofacial Surgery, 2021, 31(3): 177-179. doi: 10.3969/j.issn.1005-4979.2021.03.009 [6] 王鹏程, 陈春晖, 童熹, 等. β-TCP植入与口腔修复膜覆盖治疗对颌骨囊肿术后骨缺损的修复效果分析[J]. 口腔医学研究, 2021, 37(3): 260-263. https://www.cnki.com.cn/Article/CJFDTOTAL-KQYZ202103023.htmWANG P C, CHEN C H, TONG X, et al. Effect ofβ-TCP combined with oral repair membrane on bone defect restoration after jaw cyst excision[J]. Journal of Oral Science Research, 2021, 37(3): 260-263. https://www.cnki.com.cn/Article/CJFDTOTAL-KQYZ202103023.htm [7] 范永晶, 金武龙, 刘莹. 200例颌骨囊性病变临床回顾分析[J]. 中国口腔颌面外科杂志, 2019, 17(3): 269-274. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGKQ201903026.htmFAN Y J, JIN W L, LIU Y. Clinical retrospective analysis of 200 cases with cystic lesions of the jaw bone[J]. China Journal of Oral and Maxillofacial Surgery, 2019, 17(3): 269-274. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGKQ201903026.htm [8] 王涛. 开窗减压联合二期磨刮术治疗下颌骨大型嚢性成釉细胞瘤效果观察[J]. 中华实用诊断与治疗杂志, 2017, 31(3): 259-261. https://www.cnki.com.cn/Article/CJFDTOTAL-HNZD201703016.htmWANG T. Effect of fenestration combined with second curettage on mandibular giant cystic ameloblastoma[J]. Journal of Chinese Practical Diagnosis and Therapy, 2017, 31(3): 259-261. https://www.cnki.com.cn/Article/CJFDTOTAL-HNZD201703016.htm [9] 冯燕平, 程鹏, 朱保玉. 开窗减压术治疗大型颌骨囊性病变39例临床观察[J]. 医药论坛杂志, 2019, 40(5): 58-59, 62. https://www.cnki.com.cn/Article/CJFDTOTAL-HYYX201905019.htmFENG Y P, CHENG P, ZHU B Y. Clinical observation of fenestration decompression in treatment of large jaw cystic lesions[J]. Journal of Medical Forum, 2019, 40(5): 58-59, 62. https://www.cnki.com.cn/Article/CJFDTOTAL-HYYX201905019.htm [10] 罗建峰, 周昊, 魏卓, 等. 牙源性颌骨囊肿的临床病理特点分析[J]. 实用医院临床杂志, 2021, 18(3): 104-107. https://www.cnki.com.cn/Article/CJFDTOTAL-YYLC202103033.htmLUO J F, ZHOU H, WEI Z, et al. Analysis of clinicopathological characteristics of odontogenic jaw cysts[J]. Practical Journal of Clinical Medicine, 2021, 18(3): 104-107. https://www.cnki.com.cn/Article/CJFDTOTAL-YYLC202103033.htm [11] 杨绍滨, 张静, 薛娇, 等. 牙源性角化囊肿上皮细胞体外培养及其生物学特性[J]. 精准医学杂志, 2019, 34(4): 345-349. https://www.cnki.com.cn/Article/CJFDTOTAL-SPAN201904017.htmYANG S B, ZHANG J, XUE J, et al. In vitro culture and biological characteristics of epithelial cells in odontogenic keratocyst[J]. Journal of Precision Medicine, 2019, 34(4): 345-349. https://www.cnki.com.cn/Article/CJFDTOTAL-SPAN201904017.htm [12] PARK H S, SONG I S, SEO B M, et al. The effectiveness of decompression for patients with dentigerous cysts, keratocystic odontogenic tumors, and unicystic ameloblastoma[J]. J Korean Assoc Oral Maxillofac Surg, 2014, 40(6): 260-265. [13] MOHANTY S, DABAS J, VERMA A, et al. Surgical management of the odontogenic keratocyst: A 20-year experience[J]. Int J Oral Maxillofac Surg, 2021, 50(9): 1168-1176. [14] MUSTANSIR-UL-HASSNAIN S, CHANDAVARKAR V, MISHRA M N, et al. Histopathologic and immunohistochemical findings of odontogenic jaw cysts treated by decompression technique[J]. J Oral Maxillofac Pathol, 2021, 25(2): 272-278. [15] 胡玲玲, 潘珲, 谢志坚. 开窗减压术治疗颌骨囊性病变的临床研究新进展[J]. 中国实用口腔科杂志, 2021, 14(2): 239-242. https://www.cnki.com.cn/Article/CJFDTOTAL-ZSKQ202102026.htmHU L L, PAN H, XIE Z J. New clinical progress in the treatment of cystic lesions of jaw with decompression[J]. Chinese Journal of Practical Stomatology, 2021, 14(2): 239-242. https://www.cnki.com.cn/Article/CJFDTOTAL-ZSKQ202102026.htm [16] GURLER G, YILMAZ S, DELIBASI C, et al. Conservative surgical treatment of the jaw cysts in children: Case study of five patients[J]. Niger J Clin Pract, 2017, 20(9): 1216-1220. -


 点击查看大图
点击查看大图
计量
- 文章访问数: 1889
- HTML全文浏览量: 590
- PDF下载量: 24
- 被引次数: 0
