

The application of horseshoe-shaped intersegmental plane processing method with energy equipment in thoracoscopic accurate pulmonary nodules segmentectomy
-
摘要:
目的 探讨能量器械马蹄铁形段间平面处理方法应用于肺部结节胸腔镜精准肺段切除术的有效性与安全性。 方法 选择2019年1月—2021年6月因肺部结节在铜陵市人民医院行胸腔镜下肺段切除手术的100例患者,采用随机数字表法分为能量器械马蹄铁形段间平面切开组(观察组)和切缝器段间平面切开组(对照组),各50例,对比分析手术前后相关临床资料。主要观察指标为术后3 d内引流量、术后肺漏气时间、动脉血气和肺功能等。 结果 2组术中出血量、手术时间、术后3 d内引流量、术后引流管留置时间、术后肺漏气时间、术后住院时间、术后并发症等指标比较差异无统计学意义(均P>0.05);观察组住院费用少于对照组(P < 0.001);术后1个月观察组动脉血气和肺功能指标显著优于对照组(均P < 0.05),观察组术后PaO2大于对照组,术后PaCO2小于对照组,观察组术后用力肺活量为(2.58±0.43)L,高于对照组的(2.21±0.34)L,观察组术后第1秒用力呼气容积为(2.32±0.39)L,高于对照组的(1.96±0.32)L,差异有统计学意义(均P < 0.05)。 结论 能量器械马蹄铁形段间平面处理方法应用于肺部结节精准肺段切除术,是一种安全、有效、肺膨胀更加良好并能节约高值耗材的方法,值得推广。 -
关键词:
- 能量器械 /
- 马蹄铁形段间平面处理方法 /
- 肺结节 /
- 肺段切除术
Abstract:Objective To explore the effectiveness and safety of the application of horseshoe-shaped intersegmental plane processing method with energy equipment in thoracoscopic accurate pulmonary nodules segmentectomy. Methods Total 100 patients underwent thoracoscopic segmentectomy for the treatment of pulmonary nodules in Tongling People ' s Hospital from January 2019 to June 2021 were randomly divided into horseshoe-shaped intersegmental plane incision group with energy equipment (observation group) and intersegmental plane incision group with cutting suture device (control group) according to the random digital table method, with 50 cases in each group. The preoperative and postoperative clinical data was compared and analyzed. The main indexes included the drainage volume within 3 days after operation, the time of pulmonary leakage, arterial blood gas and pulmonary function. Results There was no difference in indexes like intraoperative blood loss, operation time, postoperative drainage volume within 3 days, postoperative drainage tube indwelling time, postoperative pulmonary air leakage time, postoperative hospitalization time and postoperative complications between the two groups (all P>0.05). Hospitalization costs in the observation group were significantly less than those in the control group (P < 0.001). At 1 month after operation, the arterial blood gas and the pulmonary function of the observation group was significantly better than that of the control group (all P < 0.05). The postoperative PaO2 in the observation group was higher than that of the control group, the postoperative PaCO2 in the observation group was lower than that of the control group, the postoperative forced vital capacity in the observation group [(2.58±0.43) L] was higher than that of the control group [(2.21±0.34) L], and the postoperative forced expiratory volume in one second in the observation group [(2.32±0.39) L] was higher that of the control group [(1.96±0.32) L]. The differences were statistically significant (all P < 0.05). Conclusion The application of horseshoe-shaped intersegmental plane processing method with energy equipment in thoracoscopic accurate pulmonary nodules segmentectomy is a safe and effective method with better pulmonary expansion and high-value consumables saving, which is worth popularizing. -

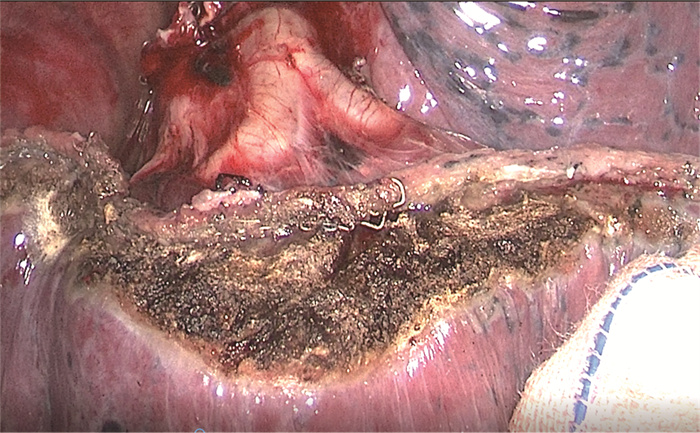
图 1 观察组马蹄铁形切开段间平面
Figure 1. Divided into the horseshoe-shaped intersegmental plane in the observation group

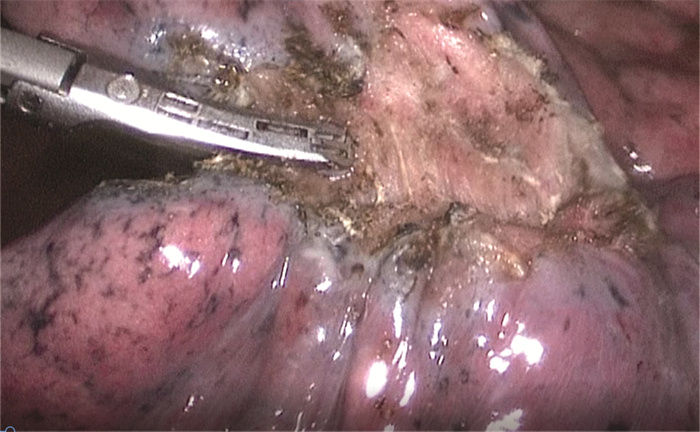
图 2 观察组马蹄铁形段间平面
Figure 2. Horseshoe shaped intersegmental plane in the observation group
表 1 2组肺部结节患者一般资料比较
Table 1. Comparison of general data between two groups
组别 例数 性别(例) 年龄(x±s,岁) BMI (x±s) 术中病理(例) 男性 女性 良性 AIS/MIA 观察组 50 19 31 57.12±12.26 23.32±1.82 5 45 对照组 50 24 26 57.90±12.67 23.36±1.86 7 43 统计量 1.020a 0.313b 0.109b 0.379a P值 0.313 0.755 0.913 0.538 注:a为χ2值,b为t值。AIS为原位腺癌(adenocarcinoma in situ),MIA为微浸润腺癌(minimally invasive adenocarcinoma)。  下载: 导出CSV
下载: 导出CSV
表 2 2组肺部结节患者肺结节所属肺段分布情况比较(例)
Table 2. Comparison of lung segment distribution of pulmonary nodules between two groups (cases)
组别 例数 右上叶 右下叶 左上叶 左下叶 S1 S2 S3 小计 S6 S7+8 S9+10 小计 S1+2 S3 S4+5 小计 S6 S7+8 S9+10 小计 观察组 50 13 6 4 23 3 1 1 5 9 2 4 15 4 2 1 7 对照组 50 10 5 4 19 4 3 1 8 7 3 7 17 4 1 1 6 χ2值 0.657 0.796 0.184 0.048 P值 0.418 0.372 0.668 0.827
下载: 导出CSV
表 3 2组肺部结节患者手术相关资料比较(x±s)
Table 3. Comparison of surgical data between two groups (x±s)
组别 例数 术中出血量(mL) 手术时间(min) 术后3 d总引流量(mL) 引流管留置时间(d) 术后漏气时间(d) 术后住院时间(d) 住院费用(元) 观察组 50 74.41±22.72 116.57±19.56 339.92±71.83 2.85±1.21 1.95±1.33 4.42±0.90 20 755.26±3 438.65 对照组 50 68.92±20.15 108.53±22.36 314.81±57.21 2.79±0.97 1.70±0.90 4.25±1.13 24 613.21±5 493.36 t值 1.278 1.913 1.934 0.274 1.100 0.832 4.209 P值 0.204 0.059 0.056 0.785 0.274 0.407 < 0.001
下载: 导出CSV
表 4 2组肺部结节患者动脉血气和肺功能指标比较(x±s)
Table 4. Comparison of arterial blood gas and pulmonary function indexes between two groups (x±s)
组别 例数 PaO2(mm Hg) PaCO2(mm Hg) FVC(L) FEV1(L) 术前 术后 术前 术后 术前 术后 术前 术后 观察组 50 85.3±11.4 76.7±17.6a 40.5±3.4 31.3±9.4a 2.84±0.35 2.58±0.43a 2.63±0.41 2.32±0.39a 对照组 50 83.2±10.5 69.3±12.3a 41.3±2.8 36.1±10.2a 2.79±0.36 2.21±0.34a 2.65±0.30 1.96±0.32a t值 0.958 2.437 1.284 2.450 0.704 4.772 0.278 5.046 P值 0.340 0.017 0.202 0.016 0.483 < 0.001 0.782 < 0.001 注:与同组术前比较,aP < 0.05。1 mm Hg=0.133 kPa。
下载: 导出CSV
-
[1] 李勤, 李伟, 沈圆兵, 等. 安徽省三级医院肺癌诊断现状分析[J]. 中华全科医学, 2018, 16(4): 518-522. doi: 10.16766/j.cnki.issn.1674-4152.000143LI Q, LI W, SHEN Y B, et al. Analysis of diagnosis status of lung cancer in tertiary hospitals in Anhui Province[J]. Chinese Journal of General Practice, 2018, 16(4): 518-522. doi: 10.16766/j.cnki.issn.1674-4152.000143 [2] NOMORI H, MORI T, SHIRAISHI A, et al. Long-term prognosis after segmentectomy for cT1 N0 M0 non-small cell lung cancer[J]. Ann Thorac Surg, 2019, 107(5): 1500-1506. doi: 10.1016/j.athoracsur.2018.11.046 [3] STILES B M, MAO J, SEBRON H, et al. Sublobar resection for node-negative lung cancer 2-5 cm in size[J]. Eur J Cardiothorac Surg, 2019, 56(5): 858-866. doi: 10.1093/ejcts/ezz146 [4] 陈刚, 汪方清, 阮卫民, 等. 能量器械与切割缝合器在肺部小结节肺段切除术的应用对比研究[J]. 临床肺科杂志, 2021, 26(4): 499-502, 508. doi: 10.3969/j.issn.1009-6663.2021.04.003CHEN G, WANG F Q, RUAN W M, et al. A comparative study on the application of energy instruments and cutting staples in pulmonary nodules segmentectomy[J]. Journal of Clinical Pulmonary Medicine, 2021, 26(4): 499-502, 508. doi: 10.3969/j.issn.1009-6663.2021.04.003 [5] 刘海波, 林钢, 张诗杰, 等. 电刀切割和机械切割在全胸腔镜肺段切除术段间平面分离中应用的对照研究[J]. 中国肺癌杂志, 2017, 20(1): 41-46. https://www.cnki.com.cn/Article/CJFDTOTAL-FAIZ201701007.htmLIU H B, LIN G, ZHANG S J, et al. Electrocautery versus stapler for intersegmental plane dissection in complete thoracoscopic segmentectomy[J]. Chinese Journal of Lung Cancer, 2017, 20(1): 41-46. https://www.cnki.com.cn/Article/CJFDTOTAL-FAIZ201701007.htm [6] MACMAHON H, NAIDICH D P, GOO J M, et al. Guidelines for management of incidental pulmonary nodules detected on CT images: From the fleischner society 2017[J]. Radiology, 2017, 284(1): 228-243. doi: 10.1148/radiol.2017161659 [7] 姜格宁, 陈昶, 朱余明, 等. 上海市肺科医院磨玻璃结节早期肺腺癌的诊疗共识(第一版)[J]. 中国肺癌杂志, 2018, 21(3): 147-159. https://www.cnki.com.cn/Article/CJFDTOTAL-FAIZ201803005.htmJIANG G N, CHEN C, ZHU Y M, et al. Shanghai pulmonary hospital experts consensus on the management of groundglass nodules suspected as lung adenocarcinoma (Version 1)[J]. Chinese Journal of Lung Cancer, 2018, 21(3): 147-159. https://www.cnki.com.cn/Article/CJFDTOTAL-FAIZ201803005.htm [8] 陈亮, 王俊, 吴卫兵, 等. 胸腔镜精准肺段切除术技术流程和质量控制[J]. 中国胸心血管外科临床杂志, 2019, 26(1): 21-28. https://www.cnki.com.cn/Article/CJFDTOTAL-ZXYX201901004.htmCHEN L, WANG J, WU W B, et al. Technical process and quality control of precise thoracoscopic lung segmentectomy[J]. Chinese Journal of Clinical Thoracic and Cardiovascular Surgery, 2019, 26(1): 21-28. https://www.cnki.com.cn/Article/CJFDTOTAL-ZXYX201901004.htm [9] TANVETYANON T, KEENAN R J. Recovery of lung function after segmentectomy versus lobectomy for early-stage lung cancer[J]. J Thorac Dis, 2018, 10(Suppl18): s2144-s2146. [10] 张新伟, 王瑞洁, 雷光焰, 等. 胸腔镜肺叶切除术与肺段切除术治疗早期肺癌的疗效观察[J]. 中国肿瘤临床与康复, 2021, 28(10): 1212-1215. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGZK202110023.htmZHANG X W, WANG R J, LEI G Y, et al. Efficacy of thoracoscopic lobectomy versus thoracoscopic segmentectomy for the treatment of early lung cancer[J]. Chinese Journal of Clinical Oncology and Rehabilitation, 2021, 28(10): 1212-1215. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGZK202110023.htm [11] 解明然, 王高祥, 徐美青, 等. 术前规划联合荧光胸腔镜精准肺段手术较传统胸腔镜肺段手术治疗早期肺腺癌近期结果比较[J]. 中国肺癌杂志, 2021, 24(7): 483-489. https://www.cnki.com.cn/Article/CJFDTOTAL-FAIZ202107005.htmXIE M R, WANG G X, XU M Q, et al. Comparison of short-term results of preoperative planning combined with fluorescence video-assisted thoracoscopic precision segmentectomy and traditional thoracoscopic segmentectomy in the treatment of early lung adenocarcinoma[J]. Chinese Journal of Lung Cancer, 2021, 24(7): 483-489. https://www.cnki.com.cn/Article/CJFDTOTAL-FAIZ202107005.htm [12] SUBRAMANIAN M, MCMURRY T, MEYERS B F, et al. Long-term results for clinical stage Ia lung cancer: Comparing lobectomy and sublobar resection[J]. Ann Thorac Surg, 2018, 106(2): 375-381. [13] 张彤, 马永富, 石渊博, 等. 荧光染色法与改良膨胀萎陷法判定段间平面在解剖性肺段切除术中的病例对照研究[J]. 中华腔镜外科杂志(电子版), 2019, 12(6): 356-360. https://www.cnki.com.cn/Article/CJFDTOTAL-ZQJW201906010.htmZHANG T, MA Y F, SHI Y B, et al. Fluorescence method versus modified inflation-deflation method distinguish intersegmental plane in thoracoscopic anatomical segmentectomy[J]. Chinese journal of laparoscopic surgery (Electronic Edition), 2019, 12(6): 356-360. https://www.cnki.com.cn/Article/CJFDTOTAL-ZQJW201906010.htm [14] MIMURA T, YAMASHITA Y, KAGIMOTO A, et al. Safety of a novel microwave surgical instrument for lung parenchyma dissection during segmentectomy[J]. Ann Thorac Surg, 2020, 109(6): 1692-1699. [15] 陈昊, 黄麟, 郑斌, 等. 单孔胸腔镜下肺段切除术中超声刀分离段间平面的应用研究[J]. 中华胸部外科电子杂志, 2019, 6(2): 131-135. https://www.cnki.com.cn/Article/CJFDTOTAL-XBWK201902010.htmCHEN H, HUANG L, ZHENG B, et al. Usefulness of an ultrasonic scalpel in segmental plane separation in single hole thoracoscopic surgery for pulmonary segmentectomy: An applied study[J]. Chinese Journal of Thoracic Surgery(Electronic Edition), 2019, 6(2): 131-135. https://www.cnki.com.cn/Article/CJFDTOTAL-XBWK201902010.htm [16] YAO F, WANG J, YAO J, et al. Early experience with video-assisted thoracoscopic anatomic segmentectomy[J]. J Laparoendosc Adv Surg Tech A, 2018, 28(7): 819-826. [17] SAGAWA M, OIZUMI H, SUZUKI H, et al. A prospective 5-year followup study after limited resection for lung cancer with ground-glass opacity[J]. Eur J Cardiothorac Surg, 2018, 53(4): 849-856. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 670
- HTML全文浏览量: 446
- PDF下载量: 3
- 被引次数: 0
