

The predictive value of systemic immune-inflammation index for intravenous immunoglobulin resistance in children with Kawasaki disease
-
摘要:
目的 评价系统免疫炎症指数(SII)对于川崎病(KD)患儿静脉注射免疫球蛋白(IVIG)治疗抵抗的预测价值。 方法 回顾性分析2018年1月—2022年3月在中国科学技术大学附属第一医院儿科诊断为KD并接受IVIG治疗的住院患儿445例,依据是否出现IVIG抵抗分为IVIG抵抗组(39例)和IVIG敏感组(406例);再依据血小板值进行分层分析。分别比较各组间炎症指标的差异;针对各差异指标,采用二元logistic回归分析研究其与KD患儿IVIG治疗抵抗的相关性;采用受试者工作特征(ROC)曲线评价各炎性指标预测KD患儿IVIG治疗抵抗的价值。 结果 整体KD患儿样本中,IVIG抵抗组较IVIG敏感组中性粒细胞(N)、中性粒细胞淋巴细胞比率(NLR)、血小板淋巴细胞比率(PLR)、SII、CRP水平高,淋巴细胞(L)较低,差异有统计学意义(均P<0.05);血小板减少KD患儿样本中,各炎症指标数值差异均无统计学意义;非血小板减少KD患儿样本中,IVIG抵抗组较IVIG敏感组N、NLR、SII水平高,差异有统计学意义(均P<0.05)。Logistic回归分析显示,整体样本和非血小板减少KD样本中,NLR与SII均为预测KD患儿IVIG治疗抵抗的因素;ROC曲线分析显示,NLR对于整体KD患儿IVIG抵抗预测敏感度为55%,特异度为67%;SII对于非血小板减少KD患儿IVIG抵抗预测敏感度为56%,特异度为64%。 结论 NLR对于整体KD患儿IVIG抵抗预测能力较强,SII对于非血小板减少KD患儿IVIG抵抗预测能力较强。 -
关键词:
- 川崎病 /
- 系统免疫炎症指数 /
- 静脉注射免疫球蛋白抵抗 /
- 血小板
Abstract:Objective To evaluate the predictive value of systemic immune-inflammation index (SII) for intravenous immunoglobulin (IVIG) resistance in children with Kawasaki disease (KD). Methods A total of 445 hospitalized children diagnosed with KD and treated with IVIG in the First Affiliated Hospital of University of Science and Technology of China from January 2018 to March 2022 were retrospectively analyzed. According to the presence of IVIG resistance, they were divided into IVIG resistance group and IVIG sensitive group. Stratified analysis was performed according to platelet value. The differences of inflammatory indexes between each group were compared and binary logistic regression was used to analyze the correlation between each inflammatory index and IVIG-resistance in children with KD. Receiver operating characteristic (ROC) curve was used to evaluate the predictive value of each inflammatory index for IVIG-resistance in children with KD. Results For all children with KD, inflammatory indexes including N, NLR, PLR, SII, and CRP of the IVIG-resistant group were higher than those of the IVIG-sensitive group (all P < 0.05), and L was lower (P < 0.05). For thrombocytopenia KD children, there was no statistical difference in the values of each inflammatory indexes. For non-thrombocytopenia KD children, the levels of N, NLR and SII of the IVIG-resistant group were higher than those of the IVIG-sensitive group (all P < 0.05). Logistic regression analysis showed that both NLR and SII were independent risk factors for predicting IVIG resistance. ROC curve analysis showed that the sensitivity of NLR for predicting IVIG-resistance in allover the KD children was 55%, and the specificity was 67%. The sensitivity of SII for predicting IVIG-resistance in non-thrombocytopenic KD children was 56%, and the specificity was 64%. Conclusion NLR has a strong predictive ability for IVIG-resistance in allover children with KD, and SII has a strong predictive ability for IVIG-resistance in non-thrombocytopenic KD children. -

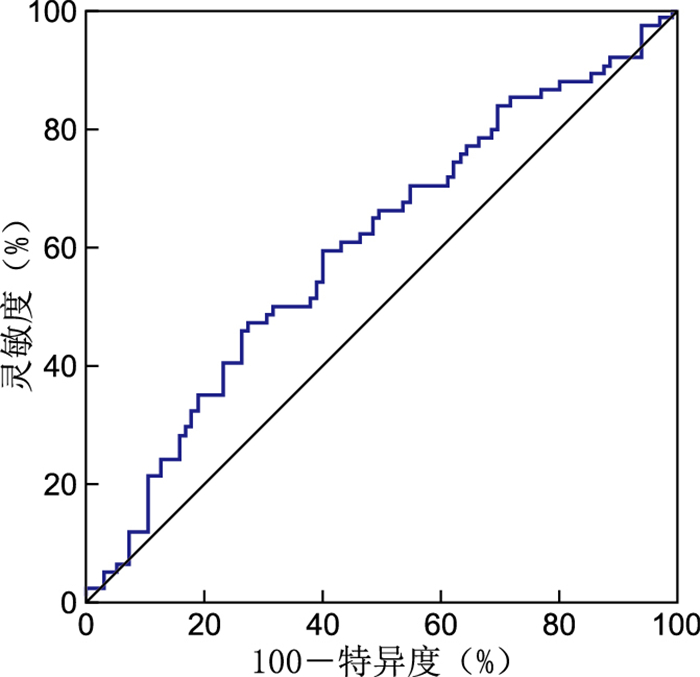
图 1 SII预测非血小板减少KD患儿IVIG抵抗的ROC曲线
Figure 1. ROC curve of SII predicting IVIG resistance in non-thrombocytopenic children with KD

图 2 SII预测整体KD患儿IVIG抵抗的ROC曲线
Figure 2. ROC curve of SII predicting IVIG resistance in overall children with KD

图 3 NLR预测整体KD患儿IVIG抵抗的ROC曲线
Figure 3. ROC curve of NLR predicting IVIG resistance in overall children with KD

图 4 NLR预测非血小板减少KD患儿IVIG抵抗的ROC曲线
Figure 4. ROC curve of NLR predicting IVIG resistance in non-thrombocytopenic children with KD
表 1 2组KD患儿一般临床资料比较
Table 1. Comparison of general clinical data of children with KD between two groups
组别 例数 年龄[M(P25, P75),岁] 性别(例) 首次IVIG治疗时间(x±s,d) 合并CAL(例) 男 女 是 否 IVIG抵抗组 39 1.83(1.00, 2.75) 24 15 6.23±1.46 14 25 IVIG敏感组 406 1.42(0.71, 2.67) 272 134 6.12±1.28 128 278 统计量 1.463a 0.133b 0.507c 0.313b P值 0.143 0.715 0.613 0.576 注:a为Z值,b为χ2值,c为t值。  下载: 导出CSV
下载: 导出CSV
表 2 2组KD患儿炎性指标比较
Table 2. Comparison of inflammatory indexes of children with KD between two groups
组别 例数 WBC [M(P25, P75),×109/L] PLT (x±s,×109/L) N [M(P25, P75),×109/L] L (x±s,×109/L) NLR [M(P25, P75)] IVIG抵抗组 39 12.04(9.49, 18.40) 317.93±150.15 10.40(6.39, 12.60) 2.18±1.07 3.68(1.68, 6.16) IVIG敏感组 406 12.13(9.23, 16.36) 288.50±143.47 8.70(4.48, 10.96) 3.27±1.72 2.66(1.15, 3.94) 统计量 0.989a 1.596b 3.056a 2.315b 2.110a P值 0.324 0.112 0.002 0.021 0.001 组别 例数 PLR[M(P25, P75)] SII[M(P25, P75)] MPV[M(P25, P75),fL] CRP(x±s,mg/L) IVIG抵抗组 39 145.41(101.23,233.22) 1 166.92(638.41, 1 883.65) 9.0(8.4, 9.9) 93.56±4.44 IVIG敏感组 406 88.07(69.32, 166.51) 737.79(345.18, 1 338.38) 9.1(8.5, 9.7) 72.49±4.02 统计量 2.332a 3.229a -0.227a 1.408b P值 0.001 0.025 0.820 0.031 注:a为Z值,b为t值。
下载: 导出CSV
表 3 2组KD患儿不同PLT分层炎性指标比较[M(P25, P75)]
Table 3. Comparison of inflammatory indexes of children with KD between two groups with different platelets stratification [M(P25, P75)]
组别 例数 血小板减少 N(×109/L) L(×109/L) NLR PLR SII CRP(mg/L) IVIG抵抗组 5 9.50(4.66, 10.12) 2.83(1.79, 3.52) 3.46(2.18, 4.98) 105.14(81.22,252.31) 630.23(338.36, 1 035.05) 73.26(33.96, 147.48) IVIG敏感组 48 8.90(5.20, 11.33) 3.09(2.05,4.92) 3.15(2.04, 4.75) 118.12(89.55, 241.09) 621.34(320.27, 1 495.36) 60.39(36.51, 120.17) Z值 -0.863a 1.152a 1.547a -1.088a 2.169a 1.985a P值 0.121 0.352 0.422 0.285 0.242 0.277 组别 例数 非血小板减少 N(×109/L) L(×109/L) NLR PLR SII CRP(mg/L) IVIG抵抗组 34 11.02(6.62, 13.11) 3.55±1.18 3.71(1.08, 2.83) 142.38(91.54,356.13) 1 555.30 (478.56, 1 348.89) 87.72±5.08 IVIG敏感组 358 8.00(4.12, 10.58) 3.70±2.10 2.24(1.62, 2.98) 158.07(89.23, 277.52) 728.88(545.09, 1 529.54) 80.56±3.52 Z值 3.512a 1.908b 1.711a 2.198a 1.766a 2.006b P值 0.002 0.092 0.001 0.315 0.001 0.099 注:a为Z值,b为t值。
下载: 导出CSV
表 4 多因素logistic回归分析变量赋值表
Table 4. Variable assignment table for multivariate logistic regression analysis
变量名称 变量赋值临界值 赋值方法 是否IVIG抵抗 是=1,否=0 N 1周岁以下或4周岁以上患儿, 是否>6.00×109/L 是=1,否=0 1~4周岁患儿,是否>4.20×109/L 是=1,否=0 CRP 是否<8.00 mg/L 是=1,否=0 L 是否<4.00×109/L 是=1,否=0 NLR 是否<3.71 是=1,否=0 PLR 是否<105.66 是=1,否=0 SII 是否<845.25 是=1,否=0
下载: 导出CSV
表 5 KD患儿IVIG治疗抵抗危险因素的多变量logistic回归分析
Table 5. Multivariate logistic regression analysis of risk factors for IVIG resistance in children with KD
PLT分层 变量 B SE Wald χ2 P值 OR值 95% CI 整体 N 0.751 0.720 1.088 0.410 0.472 0.115~1.935 L 0.794 1.034 0.590 0.517 2.212 0.292~16.788 NLR -0.160 0.168 0.907 0.038 0.852 0.613~1.184 PLR 0.783 1.101 0.506 0.075 2.187 0.253~18.934 SII -0.341 0.132 6.674 0.035 0.711 0.549~0.921 CRP 1.180 0.713 2.739 0.181 3.256 0.805~13.164 非血小板减少 N -0.796 0.723 1.212 0.342 0.451 0.109~1.861 NLR -0.533 0.263 4.119 0.042 0.587 0.352~0.982 SII 0.000 0.000 0.464 0.032 1.002 0.987~1.121
下载: 导出CSV
-
[1] 中华医学会儿科学分会心血管学组, 中华医学会儿科学分会风湿学组, 中华医学会儿科学分会免疫学组, 等. 川崎病诊断和急性期治疗专家共识[J]. 中华儿科杂志, 2022, 60(1): 6-13.The Subspecialty Group of Cardiolgy, The Society of Pediatrics, Chinese Medical Association; The Subspecialty Group of Rheumatology, The Society of Pediatrics, Chinese Medcial Association; The Subspecialty Group of Immunology, The Society of Pediatrics, Chinese Medical Association; et al. The expert consensus on diagnosis and acute-phase treatment of Kawasaki disease[J]. Chinese Journal of Pediatrics, 2022, 60(1): 6-13. [2] SOSA T, BROWER L, DIVANOVIC A. Diagnosis and management of Kawasaki disease[J]. JAMA Pediatr, 2019, 173(3): 278-279. doi: 10.1001/jamapediatrics.2018.3307 [3] ARANE K, MENDELSOHN K, MIMOUNI M, et al. Japanese scoring systems to predict resistance to intravenous immunoglobulin in Kawasaki disease were unreliable for Caucasian Israeli children[J]. Acta Pediatr, 2018, 107(12): 2179-2184. doi: 10.1111/apa.14418 [4] 陈玉萍, 张兰. 不同炎性指标检测在川崎病患儿诊断中的价值[J]. 中华全科医学, 2020, 18(3): 362-364. doi: 10.16766/j.cnki.issn.1674-4152.001247CHEN Y P, ZHANG L. The value of different inflammatory indicators in children with Kawasaki disease[J]. Chinese Journal of General Practice, 2020, 18(3): 362-364. doi: 10.16766/j.cnki.issn.1674-4152.001247 [5] YI L P, ZHANG J, ZHONG J R, et al. Elevated levels of platelet activating factor and its acetylhydrolase indicate high risk of Kawasaki disease[J]. J Interferon Cytokine Res, 2020, 40(3): 159-167. doi: 10.1089/jir.2019.0141 [6] KANAI T, TAKESHITA S, KAWAMURA Y, et al. The combination of the neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios as a novel predictor of intravenous immunoglobulin resistance in patients with Kawasaki disease: A multicenter study[J]. Heart Vessels, 2020, 35(10): 1463-1472. doi: 10.1007/s00380-020-01622-z [7] JOMRICH G, PAIREDER M, KRISTO I, et al. High systemic immune-inflammation index is an adverse prognostic factor for patients with gastroesophageal adenocarcinoma[J]. Ann Surg, 2021, 273(3): 532-541. doi: 10.1097/SLA.0000000000003370 [8] CARPIO-ORANTES L D, GAR ĆIA-MÉNDEZ S, HERNÁNDEZ-HERNÁNDEZ S N. Neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio and systemic immune-inflammation index in patients with COVID-19-associated pneumonia[J]. Gac Med Mex, 2020, 156(6): 527-531. [9] 陈芃螈, 杨超, 李刚, 等. 系统性免疫-炎症指数对川崎病患儿冠脉扩张的预测价值[J]. 中国免疫学杂志, 2020, 36(16): 2003-2006. doi: 10.3969/j.issn.1000-484X.2020.16.017CHEN P Y, YANG C, LI G, et al. Predicting Value of systemic immune-inflammation index for coronary artery dilatation in patients with Kawasaki disease[J]. Chinese Journal of Immunology, 2020, 36(16): 2003-2006. doi: 10.3969/j.issn.1000-484X.2020.16.017 [10] MCCRINDLE B W, ROWLEY A H, NEWBURGER J W, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: A scientific statement for health professionals from the American heart association[J]. Circulation, 2017, 135(17): e927-e999. [11] YANG R N, CHANG Q, MENG X C, et al. Prognostic value of systemic immune-inflammation index in cancer: A meta-analysis[J]. J Cancer, 2018, 9(18): 3295-3302. doi: 10.7150/jca.25691 [12] ISHII M, EBATO T, KATO H, et al. History and future of treatment for acute stage Kawasaki disease[J]. Korean Circ J, 2020, 50(2): 112-119. doi: 10.4070/kcj.2019.0290 [13] WU G, YUE P, MA F, et al. Neutrophil-to-lymphocyte ratio as a biomarker for predicting the intravenous immunoglobulin-resistant Kawasaki disease[J]. Medicine, 2020, 99(6): e18535. DOI: 10.1097/MD.0000000000018535. [14] ARORA K, GULERIA S, JINDAL A K, et al. Platelets in Kawasaki disease: Is this only a numbers game or something beyond?[J]. Genes Dis, 2019, 7(1): 62-66. [15] JIN J, WANG J, LU Y D, et al. Platelet-derived microparticles: A new index of monitoring platelet activation and inflammation in Kawasaki disease[J]. Indian J Pediatr, 2019, 86(3): 250-255. doi: 10.1007/s12098-018-2765-2 [16] HAN S B, LEE S Y. Macrophage activation syndrome in children with Kawasaki disease: Diagnostic and therapeutic approaches[J]. World J Pediatr, 2020, 16(6): 566-574. doi: 10.1007/s12519-020-00360-6 -



 点击查看大图
点击查看大图

计量
- 文章访问数: 589
- HTML全文浏览量: 418
- PDF下载量: 4
- 被引次数: 0
