

Incidence and influencing factors of high-output ileostomy in adults: a meta-analysis
-
摘要:
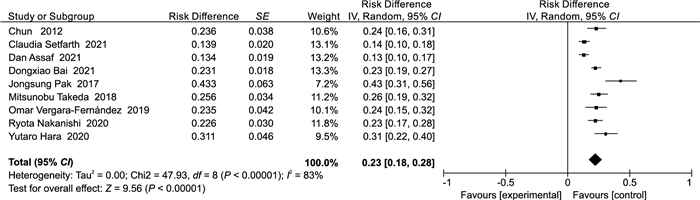
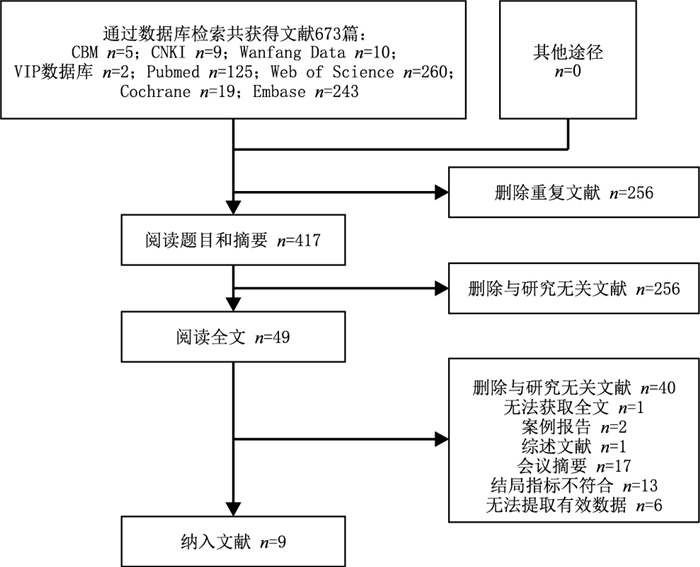
目的 系统评价高排量回肠造口(high output ileostomy,HOI)的发生率及影响因素。 方法 计算机检索CBM、CNKI、WanFang Data和VIP数据库、PubMed、Web of Science、EMbase、The Cochrane Library,检索有关HOI发生影响因素的研究文献,检索时间设置为建库至2022年5月。2名研究者独立筛选文献并提取资料,采用卡斯尔-渥太华(Newcastle-Ottawa scale,NOS)量表对文献进行偏倚风险评价。采用Review Manager 5.4统计分析。 结果 共有9项研究纳入,得分均在7分及以上。共纳入1 844例回肠造口患者,其中393例HOI,回肠造口患者的HOI总体发生率为23%(95% CI:0.18~0.28,P < 0.001)。影响因素分析结果显示,炎性肠病(OR=16.17,95% CI:7.00~37.38,P < 0.001)、糖尿病(OR=13.69,95% CI:6.42~29.20,P < 0.001)、放化疗(OR=4.50,95% CI:1.29~15.67,P=0.020)、术后出口梗阻(OR=3.77,95% CI:1.57~9.07,P=0.003)为HOI的影响因素。 结论 炎性肠病、糖尿病、放化疗及术后出口梗阻为HOI的影响因素,但现有研究数量较少,多为小样本研究,此外HOI的诊断标准不一致,在一定程度上影响meta分析结果,因此上述结论尚需进一步验证。 Abstract:Objective To perform a systematic review of the incidence and influencing factors of high-output ileostomy (HOI). Methods Computer searched CBM, CNKI, WanFang Data, VIP database, PubMed, Web of Science, EMbase, and the Cochrane Library for research literature on factors affecting the occurrence of HOI. The search time was set from the establishment of the database to May 2022. Two researchers screened the literature and extracted data independently. The Newcastle-Ottawa Scale was used to evaluate the risk of bias of the literature. Statistical analysis was performed using Review Manager 5.4. Results A total of nine studies were included, all with a score of 7 or above. In addition, 1 844 patients had ileostomy, including 393 patients with HOI. The overall incidence of HOI in patients with ileostomy was 23% (95% CI: 0.18-0.28, P < 0.001). Results of influencing factor analysis showed that inflammatory bowel disease (OR=16.17, 95% CI: 7.00-37.38, P < 0.001), diabetes (OR=13.69, 95% CI: 6.42-29.20, P < 0.001), chemoradiotherapy (OR=4.50, 95% CI: 1.29-15.67, P=0.020) and postoperative outlet obstruction (OR=3.77, 95% CI: 1.57-9.07, P=0.003) were the influencing factors of HOI. Conclusion Inflammatory bowel disease, diabetes, radiotherapy, chemoradiotherapy and postoperative outlet obstruction are the influencing factors of HOI, but the number of existing studies is small, and most of them are small sample studies. In addition, the diagnostic criteria of HOI are inconsistent, which affects the results of meta-analysis to a certain extent. Therefore, the above-mentioned conclusions must be further verified. -
Key words:
- High-output ileostomy /
- Incidence /
- Influencing factors
-
表 1 纳入文献基本特征及影响因素
Table 1. Basic characteristics and influencing factors of the included literature
作者 国家 年份 研究类型 样本量(T/C) HOI定义 影响因素 质量评价(分) ASSAF D等[7] 以色列 2021 病例对照 41/266 患者自我报告回肠造口输出量增加并伴有临床症状或实验室检验结果异常 (1)(2)(3) 7 BAI D X等[8] 中国 2021 病例对照 114/380 连续2天回肠造口输出>2 000 mL/24 h (4)(5)(6)(7)(8) 8 HARA Y等[9] 日本 2020 病例对照 32/71 连续2天回肠造口输出>1 500 mL/24 h (9) 8 NAKANISHI R等[10] 日本 2021 病例对照 44/151 回肠造口输出量≥2 000 mL/24 h (6)(10)(11)(12) 8 PAK J等[11] 日本 2017 病例对照 26/34 回肠造口输出量>1 500 mL/24 h (5) 8 SEIFARTH C等[12] 德国 2021 病例对照 41/255 回肠造口输出量每天超过1 000 mL,持续3 d以上 (4)(13)(14)(15)(16) 8 TAKEDA M等[13] 日本 2019 病例对照 42/122 回肠造口输出量>2 000 mL/24 h (5)(9)(17) 8 VERGARA-FERNÁNDEZ O等[14] 美国 2019 病例对照 24/78 回肠造口输出量>1 500 mL/24 h (4) 8 CHUN L J等[15] 美国 2012 病例对照 29/94 回肠造口输出量>2 000 mL/24 h (13)(18) 7 注:T为病例组,C为对照组;影响因素如下,(1)晚期美国麻醉医师协会全身状态分级;(2)腹腔镜手术;(3)肌酐水平;(4)炎性肠病(包括克罗恩病和炎性肠病);(5)糖尿病;(6)放化疗;(7)全结肠切除手术;(8)类固醇激素治疗;(9)出口梗阻;(10)术后Clavien-Dindo Ⅱ~Ⅳ级;(11)术后白细胞≥10 000/μL;(12)术后C-反应蛋白≥10 mg/dL;(13)年龄;(14)回肠储袋-肛管吻合手术;(15)右半结肠切除手术;(16)小肠切除手术;(17)全结直肠切除手术;(18)高血压。  下载: 导出CSV
下载: 导出CSV
-
[1] FIELDING A, WOODS R, MOOSVI S R, et al. Renal impairment after ileostomy formation: a frequent event with long-term consequences[J]. Colorectal Dis, 2020, 22(3): 269-278. doi: 10.1111/codi.14866 [2] LORIA A, MELUCCI A, SPERANZA J, et al. Acute kidney injury is a common and significant complication following ileostomy formation[J]. Colorectal Dis, 2022, 24(1): 102-110. doi: 10.1111/codi.15917 [3] LEE N, LEE S Y, KIM C H, et al. The relationship between high-output stomas, postoperative ileus, and readmission after rectal cancer surgery with diverting ileostomy[J]. Ann Coloproctol, 2021, 37(1): 44-50. doi: 10.3393/ac.2020.08.03 [4] 涂瑞沙, 蔡耀庆, 郝云鹤, 等. 加速康复外科模式下直肠癌切除术后1个月内再入院预测因素[J]. 中国老年学杂志, 2021, 41(13): 2724-2727. doi: 10.3969/j.issn.1005-9202.2021.13.012TU R S, CAI Y Q, HAO Y H, et al. Predictors of readmission within 1 month after rectal cancer resection in the accelerated rehabilitation surgical model[J]. Chinese Journal of Gerontology, 2021, 41(13): 2724-2727. doi: 10.3969/j.issn.1005-9202.2021.13.012 [5] JUSTINIANO C F, TEMPLE L K, SWANGER A A, et al. Readmissions with dehydration after ileostomy creation: rethinking risk factors[J]. Dis Colon Rectum, 2018, 61(11): 1297-1305. doi: 10.1097/DCR.0000000000001137 [6] 艾飞玲, 胡葵茹, 石钰霖, 等. 基于纽卡斯尔-渥太华量表对中国吸烟队列研究文献的质量评价[J]. 中华疾病控制杂志, 2021, 25(6): 722-729. https://www.cnki.com.cn/Article/CJFDTOTAL-JBKZ202106018.htmAI F L, HU K R, SHI Y L, et al. Quality assessment of cohort studies literature on Chinese smoking by using Newcastle-Ottawa-Scale[J]. Chinese Journal of Disease Control & Prevention, 2021, 25(6): 722-729. https://www.cnki.com.cn/Article/CJFDTOTAL-JBKZ202106018.htm [7] ASSAF D, HAZZAN D, BEN-YAACOV A, et al. Predisposing factors for high output stoma in patients with a diverting loop ileostomy after colorectal surgeries[J]. Ann Coloproctol, 2021. DOI: 10.3393/ac.2021.00241.0034. [8] BAI D X, LI L, SHEN Z L, et al. Risk factors for developing high-output ileostomy in CRC patients: a retrospective study[J]. BMC Surg, 2021, 21(1): 300. doi: 10.1186/s12893-021-01288-y [9] HARA Y, MIURA T, SAKAMOTO Y, et al. Organ/space infection is a common cause of high output stoma and outlet obstruction in diverting ileostomy[J]. BMC Surg, 2020, 20(1): 83. doi: 10.1186/s12893-020-00734-7 [10] NAKANISHI R, KONISHI T, NAKAYA E, et al. Predisposing factors and clinical impact of high-output syndrome after sphincter-preserving surgery with covering ileostomy for rectal cancer: a retrospective single-center cohort study[J]. Int J Clin Oncol, 2021, 26(1): 118-125. doi: 10.1007/s10147-020-01781-z [11] PAK J, UEMURA M, FUKUDA Y, et al. Predictors of high-output stoma after low anterior resection with diverting ileostomy for rectal cancer[J]. Int Surg, 2017, 102(7-8): 313-317. doi: 10.9738/INTSURG-D-17-00121.1 [12] SEIFARTH C, AUGUSTIN L N, LEHMANN K S, et al. Assessment of risk factors for the occurrence of a high-output ileostomy[J]. Front Surg, 2021, 8: 642288. DOI: 10.3389/fsurg.2021.642288. [13] TAKEDA M, TAKAHASHI H, HARAGUCHI N, et al. Factors predictive of high-output ileostomy: a retrospective single-center comparative study[J]. Surg Today, 2019, 49(6): 482-487. doi: 10.1007/s00595-018-1756-2 [14] VERGARA-FERNÁNDEZ O, TREJO-AVILA M, SANTES O, et al. Predictors of dehydration and acute renal failure in patients with diverting loop ileostomy creation after colorectal surgery[J]. World J Clin Cases, 2019, 7(14): 1805-1813. doi: 10.12998/wjcc.v7.i14.1805 [15] CHUN L J, HAIGH P I, TAM M S, et al. Defunctioning loop ileostomy for pelvic anastomoses: predictors of morbidity and nonclosure[J]. Dis Colon Rectum, 2012, 55(2): 167-174. doi: 10.1097/DCR.0b013e31823a9761 [16] URIBE A A, WEAVER T E, ECHEVERRIA-VILLALOBOS M, et al. Perioperative morbidity and complications in patients with an established ileostomy undergoing major abdominal surgery: a retrospective study[J]. Front Surg, 2021, 8: 757269. DOI: 10.3389/fsurg.2021.757269. [17] 中华医学会外科学分会结直肠外科学组, 中国医师协会肛肠医师分会炎症性肠病专业委员会. 中国溃疡性结肠炎外科治疗指南[J]. 中华炎性肠病杂志, 2022, 6(1): 7-16. https://www.cnki.com.cn/Article/CJFDTOTAL-ZWCW200604037.htmColorectal Surgery Group of Chinese Society of Surgery of Chinese Medical Association, Inflammatory Bowel Disease Committee of Anorectal Doctor Branch of Chinese Medical Doctor Association. Guidelines for surgical treatment of ulcerative colitis in China[J]. 中华炎性肠病杂志, 2022, 6(1): 7-16. https://www.cnki.com.cn/Article/CJFDTOTAL-ZWCW200604037.htm [18] BAKER M L, WILLIAMS R N, NIGHTINGALE J M. Causes and management of a high-output stoma[J]. Colorectal Dis, 2011, 13(2): 191-197. doi: 10.1111/j.1463-1318.2009.02107.x [19] 陈影, 程帆. 造口高排量监测及风险评估研究进展[J]. 护理研究, 2022, 36(13): 2353-2355. https://www.cnki.com.cn/Article/CJFDTOTAL-SXHZ202213017.htmCHEN Y, CHENG F. Research progress on monitoring and risk assessment of high-output stoma[J]. Chinese Nursing Research, 2022, 36(13): 2353-2355. https://www.cnki.com.cn/Article/CJFDTOTAL-SXHZ202213017.htm [20] FUJINO S, MIYOSHI N, OHUE M, et al. Prediction model and treatment of high-output ileostomy in colorectal cancer surgery[J]. Mol Clin Oncol, 2017, 7(3): 468-472. doi: 10.3892/mco.2017.1336 [21] 黄慧峰, 张艳, 陈文晓, 等. 免疫抑制剂联合生物制剂对炎症性肠病患者营养状况及炎症因子的影响[J]. 中华全科医学, 2019, 17(5): 862-864. doi: 10.16766/j.cnki.issn.1674-4152.000811HUANG H F, ZHANG Y, CHEN W X, et al. Effects of biologics combined with immunosuppressive agents on nutritional status and inflammatory response in patients with inflammatory bowel disease[J]. Chinese Journal of General Practice, 2019, 17(5): 862-864. doi: 10.16766/j.cnki.issn.1674-4152.000811 [22] 汤阿毛, 宁丽, 楼立兰, 等. 炎症性肠病个案管理师工作职责指标体系的构建[J]. 中华全科医学, 2021, 19(10): 1775-1779. doi: 10.16766/j.cnki.issn.1674-4152.002165TANG A M, NING L, LOU L L, et al. Construction of a responsibility index system of case managers for inflammatory bowel disease[J]. Chinese Journal of General Practice, 2021, 19(10): 1775-1779. doi: 10.16766/j.cnki.issn.1674-4152.002165 [23] MODI S, SYED GAGGATUR N, SANGE A H, et al. An emerging facet of diabetes mellitus: the nexus of gastrointestinal disorders[J]. Cureus, 2021, 13(9): e18245. DOI: 10.7759/cureus.18245. [24] PATEL K, HORAK H, TIRYAKI E. Diabetic neuropathies[J]. Muscle Nerve, 2021, 63(1): 22-30. [25] FENG X, LI X Q. The prevalence of small intestinal bacterial overgrowth in diabetes mellitus: a systematic review and meta-analysis[J]. Aging (Albany NY), 2022, 14(2): 975-988. [26] 桑苗苗, 吴同智, 孙子林. 糖尿病相关消化道症状的发病机制和临床诊疗进展[J]. 中华糖尿病杂志, 2021, 13(5): 513-516.SANG M M, WU T Z, SUN Z L. Pathogenesis and clinical management of diabetes-related gastrointestinal symptoms[J]. Chinese Journal of Diabetes Mellitus, 2021, 13(5): 513-516. [27] TAKAHASHI J, TSUJINAKA S, MAEMOTO R, et al. Tolerability and adverse events of adjuvant chemotherapy for rectal cancer in patients with diverting ileostomy[J]. In Vivo, 2020, 34(6): 3399-3406. [28] GARCZYK A, KALICIAK I, DROGOWSKI K, et al. Influence of probiotics in prevention and treatment of patients who undergo chemotherapy or/and radiotherapy and suffer from mucositis, diarrhoea, constipation, nausea and vomiting[J]. J Clin Med, 2022, 11(12): 3412. DOI: 10.3390/jcm11123412. [29] FENG J, GAO M, ZHAO C C, et al. Oral administration of probiotics reduces chemotherapy-induced diarrhea and oral mucositis: a systematic review and meta-analysis[J]. Front Nutr, 2022, 9: 823288. DOI: 10.3389/fnut.2022.823288. [30] SASAKI S, NAGASAKI T, OBA K, et al. Risk factors for outlet obstruction after laparoscopic surgery and diverting ileostomy for rectal cancer[J]. Surg Today, 2021, 51(3): 366-373. -

 点击查看大图
点击查看大图
图(3) / 表(1)
计量
- 文章访问数: 1136
- HTML全文浏览量: 849
- PDF下载量: 21
- 被引次数: 0
