

CT imaging diagnosis of primary pulmonary mucinous adenocarcinoma
-
摘要:
目的 探讨原发性肺黏液腺癌的CT影像特征并进行总结,通过其影像特点早期诊断疾病,从而选择合适的治疗手段,以此来提高生存期。 方法 选取安徽省胸科医院2019年8月—2022年8月经病理证实的62例原发性肺黏液腺癌,回顾性分析其临床、影像特征及病理结果,对原发性肺黏液腺癌的结节/肿块型与实变型两种类型的影像特征作出对照,并通过影像表现结合病理及免疫组化特征进行总结。 结果 62例患者发病年龄为14~80(60.5±10.5)岁,以咳白黏痰为主诉。影像结果示62例患者中结节/肿块型46例,其中纯磨玻璃结节2例(4.3%),混杂磨玻璃结节22例(47.8%),实性结节及肿块22例(47.8%),发生于两肺下叶胸膜下(重力较大部位)31例(67.4%),发生气道播散2例(4.3%),其他常见征象有血管集束征、空泡/空洞征等。实变型16例,发生于两肺下叶胸膜下14例(87.5%),发生气道播散9例(56.3%),其他常见征象有空泡/空洞征、血管漂浮征、枯树枝征等。病理结果示:镜下可见丰富的黏液,内见散在异型细胞团,免疫组化示:CK7(+)43例,TTF-1(+)51例,Napsin-A(+)36例,Ki-67(≤50%)53例,CDX-2(+)18例。 结论 原发性肺黏液腺癌影像上大体分为结节/肿块型及实变型两类,以肺叶重力较大位置分布为主,增强后轻到中度强化,病理见散在异型细胞团周围充满黏液成分,免疫组化诊断常见CK7(+)和TTF-1(+)。 Abstract:Objective To investigate and summarize the CT imaging characteristics of primary pulmonary mucinous adenocarcinoma, diagnose the disease early through its imaging characteristics, and select appropriate treatment methods, so as to improve survival. Methods A total of 62 cases of pathologically confirmed primary pulmonary mucinous adenocarcinoma from August 2019 to August 2022 in Anhui Provincial Chest Hospital were selected, their clinical, imaging features and pathological results were retrospectively analyzed, and the imaging features of nodular/mass type and consolidation type of primary pulmonary mucinous adenocarcinoma were compared, and the imaging manifestations combined with pathological features were summarized. Results The age of onset of 62 patients was 14-80 years old, and the average age was (60.5±10.5) years. The main complaint was cough white phlegm. The imaging results showed that there were 46 cases of nodular/mass type in 62 patients, including 2 cases (4.3%) of pure ground-glass nodules, 22 cases (47.8%) of mixed ground-glass nodules, 22 cases (47.8%) of solid nodules and masses, 31 cases (67.4%) of subpleural (gravity-heavy parts) of the lower lobes of both lungs, 2 cases occurred in airway dissemination (4.3%), and other common signs included vascular cluster sign, vacuole/cavitation sign, etc. There were 16 cases of consolidation type, with 14 cases (87.5%) occurring under the pleura in the lower lobes of both lungs, 9 cases (56.3%) experiencing airway spread, and other common signs including vacuole/cavity sign, vascular floating sign, and dead tree branch sign. The pathological results showed that abundant mucus could be seen under the microscope, scattered in the heterotypic cell mass, and the immunohistochemistry showed: CK7(+) 43 cases, TTF-1(+) 51 cases, Napsin-A (+) 36 cases, Ki-67 (≤ 50%) 53 cases, and CDX-2 (+) 18 cases. Conclusion Primary pulmonary mucinous adenocarcinoma is generally divided into nodular/mass type and consolidation type, mainly distributed in the large position of gravity of lung lobes, light to moderate reinforcement after enhancement, pathological scattered around the heterotypic cell mass filled with mucus components, and immunohistochemical diagnosis commonly involves CK7(+) and TTF-1(+). -
Key words:
- Primary pulmonary mucinous adenocarcinoma /
- Caseous pneumonia /
- Mucus lake
-

图 1 右肺下叶黏液腺癌影像学与病理
注:男性,14岁,A示右肺下叶类结节实性病灶内见空泡/空洞征;B、C示两肺多发播散病灶;D示MPR冠状位见右肺下叶病灶呈膨胀性生长;E为穿刺病理示异型细胞周围见黏液成分(HE染色,×200)。
Figure 1. Imaging and pathology of mucinous adenocarcinoma of the right lower lobe of the lung

图 2 左肺下叶黏液腺癌影像学与病理
注:男性,55岁,A、B示横断位、矢状位见左肺下叶空洞型结节灶;C示最小密度投影示空洞壁较薄;D示CT引导下经皮肺穿刺活检;E为穿刺病理示肺黏液腺癌(HE染色,×200)。
Figure 2. Imaging and pathology of mucinous adenocarcinoma of the left lower lobe of the lung

图 3 右肺上叶黏液腺癌影像学与病理
注:男性,50岁,A、B示右肺上叶近肺门结节灶,边缘分叶毛刺;C、D示测得实性部分平均CT值约40 HU;E为手术病理提示黏液腺癌(HE染色,×200)。
Figure 3. Imaging and pathology of mucinous adenocarcinoma in the upper lobe of the right lung

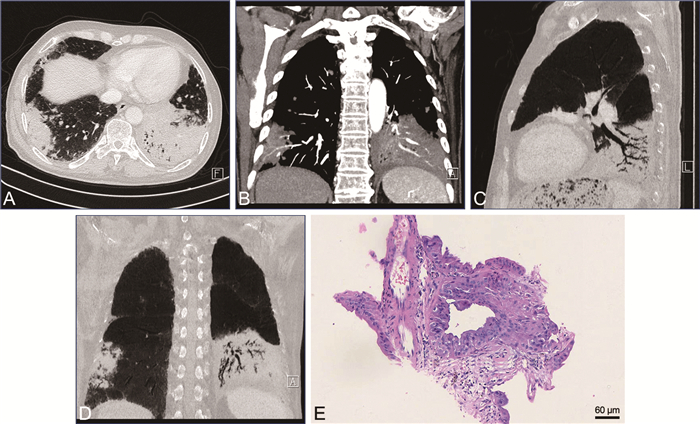
图 4 肺黏液腺癌肺内播散影像学与病理
注:男性,70岁,A示两肺下叶实变影,并可见肺内播散灶;B示增强后动脉期左肺下叶实变病灶内见强化的血管漂浮影;C、D示最小密度投影见枯树枝征;E为穿刺病理示肺黏液腺癌(HE染色,×200)。
Figure 4. Imaging and pathology of intrapulmonary dissemination of pulmonary mucinous adenocarcinoma
表 1 62例PPMA(结节/肿块型及实变型)的影像征象情况[例(%)]
Table 1. Image findings of 62 PPMA (nodule/mass type and solid type)[cases (%)]
影像特征 结节/肿块型 实变型 纯磨玻璃结节 2(4.3) 混杂磨玻璃结节 22(47.8) 7(43.8) 实性结节 22(47.8) 9(56.3) 分叶 32(69.6) 毛刺 17(36.9) 空泡/空洞征 21(45.7) 12(75.0) 血管集束征 29(63.0) 血管漂浮征 14(87.5) 枯树枝征 2(4.3) 11(68.8) 气道播散 2(4.3) 9(56.3) 胸膜增厚 34(73.9) 14(87.5)  下载: 导出CSV
下载: 导出CSV
表 2 62例PPMA免疫组化阳性标记物结果[例(%)]
Table 2. Results of PPMA immunohistochemical positive markers in 62 cases [cases (%)]
免疫组化标记物 原发性肺黏液腺癌 CK7 43(69.4) TTF-1 51(82.3) Napsin-A 36(58.1) Ki-67(≤50%) 53(85.5) CDX-2 18(29.0)
下载: 导出CSV
-
[1] HAN Y P, LUO Y J. Primary lung invasive adenocarcinoma misdiagnosed as infectious pneumonia in 18F-FDG PET/CT: a case report[J]. Radiol Case Rep, 2021, 17(3): 808-811. [2] 李媛, 谢惠康, 武春燕. WHO胸部肿瘤分类(第5版)中肺肿瘤部分解读[J]. 中国癌症杂志, 2021, 31(7): 574-580. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGAZ202109001.htmLI Y, XIE H K, WU C Y. Interpretation of lung tumors in WHO classification of thoracic tumors (5th edition)[J]. Chinese Journal of Oncology, 2021, 31(7): 574-580. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGAZ202109001.htm [3] 邵元伟, 滕敏敏, 王晓蕾, 等. 原发性肺浸润性黏液腺癌的临床病理特征与CT表现[J]. 中国临床医学影像杂志, 2020, 31(10): 719-722, 726. https://www.cnki.com.cn/Article/CJFDTOTAL-LYYX202010011.htmSHAO Y W, TENG M M, WANG X L, et al. Clinicopathological features and CT findings of primary pulmonary invasive mucinous adenocarcinoma[J]. Chinese Journal of Clinical Medical Imaging, 2020, 31(10): 719-722, 726. https://www.cnki.com.cn/Article/CJFDTOTAL-LYYX202010011.htm [4] 包杰, 金银华, 华奇峰, 等. 结合病理对原发性肺粘液腺癌的MSCT表现分析[J]. 医学影像学杂志, 2020, 30(5): 871-874. https://www.cnki.com.cn/Article/CJFDTOTAL-XYXZ202005042.htmBAO J, JIN Y H, HUA Q F, et al. Analysis of MSCT manifestations of primary pulmonary mucinous adenocarcinoma combined with pathology[J]. Journal of Medical Imaging, 2020, 30(5): 871-874. https://www.cnki.com.cn/Article/CJFDTOTAL-XYXZ202005042.htm [5] 孙伟, 于跃, 李俊, 等. 肺浸润性黏液腺癌的病理影像学特征及治疗方法应用研究进展[J]. 山东医药, 2022, 62(15): 103-107. https://www.cnki.com.cn/Article/CJFDTOTAL-SDYY202215024.htmSUN W, YU Y, LI J, et al. Research progress on pathologic imaging features and therapeutic methods of pulmonary invasive mucinous adenocarcinoma[J]. Shandong Medical Journal, 2022, 62(15): 103-107. https://www.cnki.com.cn/Article/CJFDTOTAL-SDYY202215024.htm [6] SHENG A Z, ZHOU P F, YE Y Z, et al. Diagnostic efficacy of CT radiomic features in pulmonary invasive mucinous adenocarcinoma[J]. Scanning, 2022, 2022: 5314225. DOI: 10.1155/2022/5314225. [7] 杨昭, 王小雷, 李淑华, 等. CT影像组学列线图评估肺腺癌脏层胸膜侵犯[J]. 中国医学影像技术, 2022, 38(7): 1017-1022. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXX202207012.htmYANG Z, WANG X L, LI S H, et al. Identification of pleural invasion of the visceral layer of lung adenocarcinoma by CT radiomics[J]. Chinese Journal of Medical Imaging Technology, 2022, 38(7): 1017-1022. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXX202207012.htm [8] MIYATA N, ENDO M, NAKAJIMA T, et al. High-resolution computed tomography findings of early mucinous adenocarcinomas and their pathologic characteristics in 22 surgically resected cases[J]. Eur J Radiol, 2015, 84(5): 993-997. [9] 张俊杰, 郝李刚, 许茜, 等. 基于临床及CT特征构建预测肺浸润性黏液腺癌的机器学习模型[J]. 中华全科医学, 2023, 21(1): 6-9, 49. doi: 10.16766/j.cnki.issn.1674-4152.002799ZHANG J J, HAO L G, XU Q, et al. Construction of a machine learning model for predicting lung invasive mucinous adenocarcinoma based on clinical and CT features[J]. Chinese Journal of General Practice, 2023, 21(1): 6-9, 49. doi: 10.16766/j.cnki.issn.1674-4152.002799 [10] 范真真, 高鹏. 肺炎型浸润性黏液型腺癌的CT和病理学特征分析[J]. 实用放射学杂志, 2022, 38(7): 1096-1099.FAN Z Z, GAO P. CT and pathological features of invasive mucinous adenocarcinoma pneumoniae[J]. Journal of Practical Radiology, 2022, 38(7): 1096-1099. [11] ZHOU C, ZHAO J K, SHAO J C, et al. Prognostic relevance of TTF-1 expression in stage I adenocarcinoma[J]. Oncotarget, 2017, 8(64): 107462-107468. DOI: 10.18632/oncotarget.22489. [12] 刘标, 周晓军. 非小细胞肺癌免疫组化标志物专家共识(2014)[J]. 临床与实验病理学杂志, 2015, 31(5): 481-487. https://www.cnki.com.cn/Article/CJFDTOTAL-LSBL201505001.htmLIU B, ZHOU X J. Expert consensus on immunohistochemical markers for non-small cell lung cancer (2014)[J]. Journal of Clinical and Experimental Pathology, 2015, 31(5): 481-487. https://www.cnki.com.cn/Article/CJFDTOTAL-LSBL201505001.htm [13] 王彩霞, 王晓, 吕淑慧, 等. TTF-1、SP-A在肺腺癌诊断及鉴别诊断中的价值[J]. 临床与实验病理学杂志, 2008, 24(3): 280-283. https://www.cnki.com.cn/Article/CJFDTOTAL-LSBL200803010.htmWANG C X, WANG X, LYU S H, et al. Value of TTF-1 and SP-A in the diagnosis and differential diagnosis of lung adenocarcinoma[J]. Journal of Clinical and Experimental Pathology, 2008, 24(3): 280-283. https://www.cnki.com.cn/Article/CJFDTOTAL-LSBL200803010.htm [14] 韩高华, 周晓军, 孟奎, 等. TTF-1在肺腺癌中的表达及其诊断意义[J]. 临床与实验病理学杂志, 2002, 18(6): 595-597. https://www.cnki.com.cn/Article/CJFDTOTAL-LSBL200206004.htmHAN G H, ZHOU X J, MENG K, et al. Expression and diagnostic significance of TTF-1 in lung adenocarcinoma[J]. Journal of Clinical and Experimental Pathology, 2002, 18(6): 595-597. https://www.cnki.com.cn/Article/CJFDTOTAL-LSBL200206004.htm [15] XU X L, SHEN W M, WANG D, et al. Clinical features and prognosis of resectable pulmonary primary invasive mucinous adenocarcinoma[J]. Transl Lung Cancer Res, 2022, 11(3): 420-431. [16] NIE K, NIE W, ZHANG Y X, et al. Comparing clinicopathological features and prognosis of primary pulmonary invasive mucinous adenocarcinoma based on computed tomography findings[J]. Cancer Imaging, 2019, 19(1): 47. [17] 留永健, 李霁, 王世波, 等. 晚期肺炎型肺癌: 一项中国单中心临床-放射-病理特征回顾性研究及预后分析[J]. 中国肺癌杂志, 2019, 22(6): 329-335. https://www.cnki.com.cn/Article/CJFDTOTAL-FAIZ201906001.htmLIU Y J, LI J, WANG S B, et al. Advanced pneumonic lung cancer: a retrospective study and prognostic analysis of single-center clinical-radiopathological features in China[J]. Chinese Journal of Lung Cancer, 2019, 22(6): 329-335. https://www.cnki.com.cn/Article/CJFDTOTAL-FAIZ201906001.htm [18] NAGASAKA M, POTUGARI B, NGUYEN A, et al. KRAS inhibitors- yes but what next? Direct targeting of KRAS- vaccines, adoptive T cell therapy and beyond[J]. Cancer Treat Rev, 2021, 101: 102309. DOI: 10.1016/j.ctrv.2021.102309. [19] WANG T T, YANG Y, LIU X Y, et al. Primary invasive mucinous adenocarcinoma of the lung: prognostic value of CT Imaging features combined with clinical factors[J]. Korean J Radiol, 2021, 22(4): 652-662. -



 点击查看大图
点击查看大图

计量
- 文章访问数: 1332
- HTML全文浏览量: 686
- PDF下载量: 23
- 被引次数: 0
