

The correlation between metabolic syndrome and its components with the degree of coronary artery stenosis and clinical outcomes in patients with acute myocardial infarction
-
摘要:
目的 探讨代谢综合征(MS)与急性心肌梗死(AMI)患者冠状动脉病变程度及预后的相关性。 方法 选取2019年1月—2020年12月期间新疆维吾尔自治区人民医院心内科救治的726例AMI患者作为研究对象,Gensini评分用以定量评估冠脉病变程度,终点事件定义为主要心血管不良事件(MACEs)的发生。采用多重线性回归分析研究MS及各组分与Gensini评分的相关性;采用多因素Cox回归分析研究MACEs发生的独立危险因素。 结果 MS组348例(47.9%),非MS组378例(52.1%)。与非MS组相比,MS组年龄更大,合并高血压、糖尿病、腹型肥胖、血脂异常比例更高,腰围、收缩压、空腹血糖、血尿素氮、低密度脂蛋白胆固醇、Gensini评分水平更高,血红蛋白水平较低,氯吡格雷服用比例更高,MACEs发生率更高,差异均有统计学意义(P < 0.05)。组分内比较发现:腹型肥胖组和空腹血糖升高组的Gensini评分显著升高,差异均有统计学意义(P < 0.05)。多重线性回归分析结果显示:空腹血糖升高和腹型肥胖与Gensini评分呈独立相关。多因素Cox回归分析结果显示:糖尿病和腹型肥胖是MACEs发生的独立危险因素。 结论 AMI患者合并MS十分常见,糖代谢异常和腹型肥胖与冠脉病变程度密切相关,并且明显影响患者预后。 Abstract:Objective To explore the correlation between metabolic syndrome (MS) with the degree of coronary artery stenosis and prognosis in patients with acute myocardial infarction (AMI). Methods There were 726 AMI patients as the subjects, from the Cardiology Department of Xinjiang Uygur Autonomous Region People's Hospital from January 2019 to December 2020. The Gensini score was used to quantitatively assess the degree of coronary artery stenosis and the clinical outcome was defined as major adverse cardiovascular events (MACEs). Multiple linear regression was used to analyze the correlation between MS and its components between Gensini score. Multivariate Cox regression was used to analyze the independent risk factors for MACEs. Results There were 348 patients (47.9%) in the MS group and 378 patients (52.1%) in the non-MS group. Compared with the non-MS group, patients in the MS group were older and had more combined hypertension, diabetes, abdominal obesity, dyslipidemia. Waist circumference, systolic blood pressure, fasting blood glucose, blood urea nitrogen, low density lipoprotein cholesterol and Gensini score were higher, hemoglobin levels were lower, clopidogrel utilization rate was higher and the incidence of MACEs was higher, the differences were statistically significant (P < 0.05). Internal comparison showed that Gensini scores were significantly increased in the group of abdominal obesity and elevated fasting blood glucose (P < 0.05). Multiple linear regression analysis results showed that elevated fasting blood glucose and abdominal obesity were independently correlated with Gensini score. Multivariate Cox regression analysis results showed that: diabetes and abdominal obesity were the independent risk factors for MACEs. Conclusion Patients with AMI complicated by MS were very common. Abnormal glucose metabolism and abdominal obesity were closely related to the degree of coronary artery stenosis, and significantly affect the prognosis of patients. -

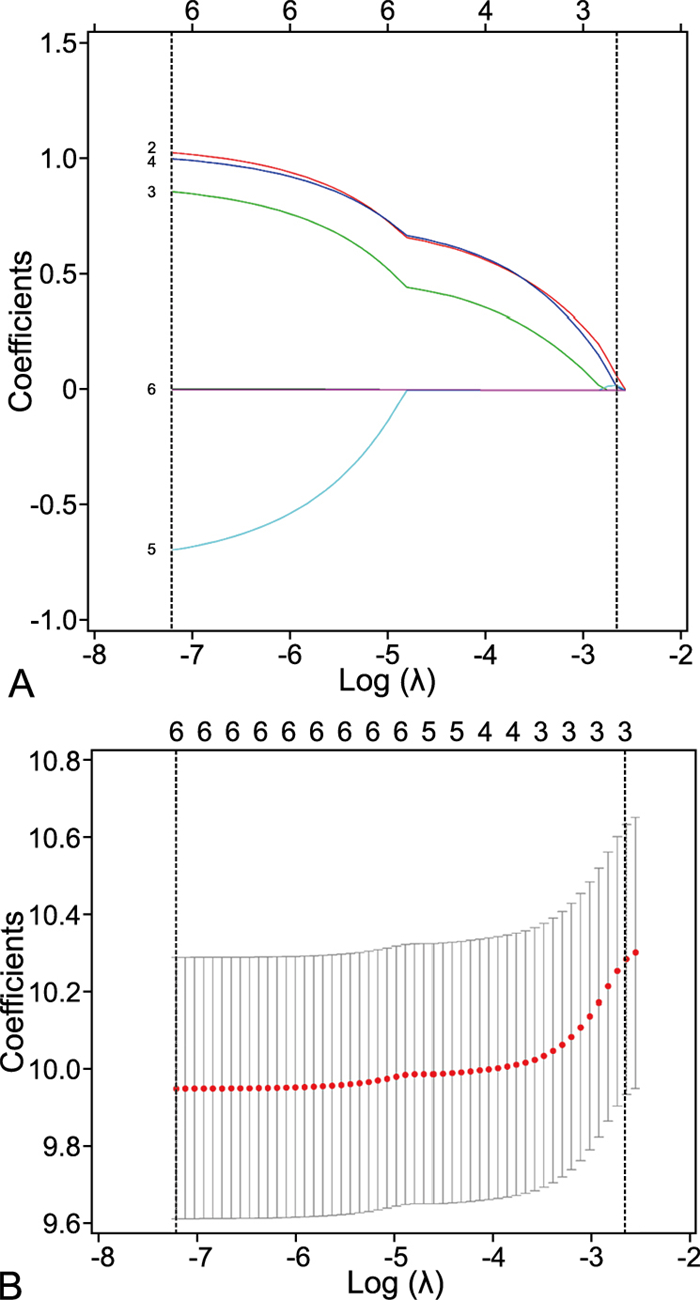
图 1 MACEs风险因素的LASSO回归筛查结果
注:A为LASSO回归的系数路径图,B为LASSO回归的交叉验证图。两条虚垂线分别为最优Lambda参数取值(Lambda.min=0.000 734 63和Lambda.1se=0.070 124 06)时,所纳入LASSO回归模型的MACEs发生的风险因素数目。
Figure 1. LASSO regression results of risk factors in MACEs
表 1 2组AMI患者基线资料比较
Table 1. Comparison of baseline data between the two groups of AMI patients
项目 MS组(n=348) 非MS组(n=378) 统计量 P值 年龄[M(P25, P75), 岁] 63.0(54.0, 70.0) 58.0(49.2, 65.0) -5.280a < 0.001 男性[例(%)] 247(71.0) 281(74.3) 1.032b 0.351 高血压[例(%)] 310(89.1) 103(27.2) 282.447b < 0.001 糖尿病[例(%)] 239(68.7) 45(11.9) 245.221b < 0.001 腹型肥胖[例(%)] 209(60.1) 80(21.2) 114.388b < 0.001 血脂异常[例(%)] 346(99.4) 333(88.1) 38.415b < 0.001 吸烟史[例(%)] 118(33.9) 152(40.2) 3.082b 0.093 冠状动脉性疾病家族史[例(%)] 59(17.0) 44(11.6) 4.202b 0.052 腰围[M(P25, P75), cm] 88.0(67.4, 100.0) 72.0(62.0, 83.6) -8.016a < 0.001 SBP[M(P25, P75), mmHg] 130(119, 143) 124(111, 136) -3.644a < 0.001 DBP[M(P25, P75), mmHg] 78(70, 85) 75.0(70, 81) -1.793a 0.073 RBC[M(P25, P75), ×1012/L] 4.53(4.19, 4.90) 4.56(4.19, 4.91) -0.389a 0.697 WBC[M(P25, P75), ×109/L] 7.12(5.90, 8.44) 7.04(5.80, 8.51) -0.358a 0.720 NE[M(P25, P75), %] 4.30(3.36, 5.37) 4.21(3.25, 5.58) -0.517a 0.605 LY[M(P25, P75), %] 1.93(1.52, 2.43) 1.96(1.51, 2.48) -0.220a 0.826 Hb[M(P25, P75), g/L] 137(127, 148) 140(130, 150) -2.153a 0.031 FBG[M(P25, P75), mmol/L] 6.72(5.19, 9.17) 5.37(4.63, 6.87) -7.481a < 0.001 BUN[M(P25, P75), nmol/L] 5.70(4.69, 6.79) 5.10(4.20, 6.30) -4.539a < 0.001 UA[M(P25, P75), nmol/L] 328(275, 396) 322(267, 389) -0.943a 0.346 TG[M(P25, P75), mmol/L] 1.65(1.19, 2.53) 1.56(1.09, 2.27) -1.951a 0.051 TC[M(P25, P75), mmol/L] 4.00(3.22, 4.79) 3.79(3.19, 4.50) -1.775a 0.076 HDL-C[M(P25, P75), mmol/L] 0.94(0.82, 1.18) 0.96(0.79, 1.13) -1.085a 0.278 LDL-C[M(P25, P75), mmol/L] 2.49(1.88, 3.13) 2.34(1.80, 2.89) -2.107a 0.035 TBIL[M(P25, P75), nmol/L] 11.50(8.48, 14.60) 11.30(8.20, 14.70) -0.271a 0.786 Gensini评分[M(P25, P75), 分] 25.0(10.8, 56.5) 20.0(6.3, 44.0) -3.210a < 0.001 随访时间[M(P25, P75), 月] 12.4(6.8, 18.9) 13.2(7.9, 19.2) -0.889a 0.374 MACEs[例(%)] 81(23.3) 57(15.1) 6.236b 0.020 阿司匹林[例(%)] 231(66.4) 256(67.7) 0.149b 0.759 氯吡格雷[例(%)] 127(36.5) 105(27.8) 6.331b 0.015 他汀类[例(%)] 202(58.0) 194(51.3) 3.303b 0.081 ACEI/ARB[例(%)] 100(28.7) 82(21.7) 0.459b 0.336 Β受体阻滞剂[例(%)] 146(42.0) 154(40.7) 0.110b 0.798 注:a为Z值,b为χ2值。NE为中性粒细胞(neutrophil),LY为淋巴细胞(lymphocyte),UA为尿酸(uric acid),TBIL为总胆红素(total bilirubin),ACEI为血管紧张素转化酶抑制剂(angiotensin converting enzyme inhibitor),ARB为血管紧张素Ⅱ受体阻滞剂(angiotensinⅡreceptor blocker)。  下载: 导出CSV
下载: 导出CSV
表 2 MS及各组分AMI患者Gensini评分比较[M(P25, P75), 分]
Table 2. Comparison of Gensini scores in patients with MS and each component of AMI patients [M(P25, P75), points]
组别 例数 Gensini评分 Z值 P值 MS组 348 25.0(10.8, 56.5) -3.210 0.001 非MS组 378 20.0(6.3, 44.0) 高血压组 413 22.0(10.0, 52.0) -1.567 0.117 非高血压组 313 20.0(7.0, 48.0) 糖尿病组 284 23.5(10.0, 56.0) -1.817 0.069 非糖尿病组 442 20.0(8.0, 44.0) FBG正常组 384 19.5(7.0, 44.0) -2.131 0.033 FBG升高组 342 24.0(10.0, 56.0) 腹型肥胖组 289 25.0(10.0, 57.0) -2.656 0.008 非腹型肥胖组 437 20.0(7.0, 44.0) HDL-C降低组 630 22.0(9.0, 49.0) -1.718 0.086 HDL-C正常组 96 15.0(5.0, 50.0) TG正常组 391 20.0(7.5, 52.0) -0.095 0.924 TG升高组 335 22.0(9.5, 45.0)
下载: 导出CSV
表 3 MS及其各组分与Gensini评分的线性回归分析
Table 3. Linear regression analysis between MS components and Gensini scores
变量 简单线性回归分析 多重线性回归分析 B SE B' t值 P值 B SE B' t值 P值 MS 8.040 2.705 0.110 2.972 0.003 高血压 2.881 2.743 0.039 1.050 0.294 糖尿病 4.554 2.781 0.061 1.638 0.102 FBG升高 5.963 2.715 0.081 2.196 0.028 6.269 2.698 0.086 2.323 0.020 腹型肥胖 8.793 2.758 0.118 3.188 0.001 9.014 2.752 0.121 3.276 0.001 HDL-C降低 3.639 4.011 0.034 0.907 0.365 TG升高 2.425 2.726 0.033 0.889 0.374
下载: 导出CSV
表 4 MS及其各组分与MACEs的Cox回归分析
Table 4. Cox regression analysis of MS components and MACEs
变量 单因素回归分析结果 多因素回归分析结果 B SE Waldχ2 HR(95% CI) P值 B SE Waldχ2 HR(95% CI) P值 年龄 0.015 0.008 1.970 1.016(1.000~1.031) 0.049 MS 0.840 0.183 4.591 2.316(1.618~3.314) < 0.001 0.070 0.251 0.280 1.073(0.656~1.756) 0.779 高血压 0.748 0.188 3.987 2.114(1.463~3.054) < 0.001 糖尿病 0.805 0.173 4.652 2.236(1.593~3.139) < 0.001 0.796 0.221 3.601 2.217(1.437~3.420) < 0.001 FBG升高 0.036 0.171 0.213 1.037(0 742~1.449) 0.831 腹型肥胖 0.755 0.174 4.339 2.127(1.513~2.992) < 0.001 0.761 0.198 3.840 2.140(1.451~3.155) < 0.001 HDL-C降低 0.292 0.267 1.096 1.339(0.794~2.259) 0.273 TG升高 -0.114 0.173 -0.659 0.892(0.636~1.252) 0.510 Gensini评分 0.004 0.002 1.886 1.004(1.000~1.008) 0.059
下载: 导出CSV
-
[1] 陈丹丹, 张慧, 邵静, 等. 代谢综合征患者饮食和运动管理方案最佳证据总结[J]. 浙江大学学报(医学版), 2022, 51(1): 27-37. https://www.cnki.com.cn/Article/CJFDTOTAL-ZJYB202201004.htmCHEN D D, ZHANG H, SHAO J, et al. Summary of the best evidence of diet and physical activity management in patients with metabolic syndrome[J]. Journal of Zhejiang University(Medical Sciences), 2022, 51(1): 27-37. https://www.cnki.com.cn/Article/CJFDTOTAL-ZJYB202201004.htm [2] LIU J, LIU Q, LI Z, et al. Prevalence of metabolic syndrome and risk factors among chinese adults: results from a population-based study-Beijing, China, 2017-2018[J]. China CDC Wkly, 2022, 4(29): 640-645. [3] 费丽萍, 周忠贤, 张容, 等. 泸州市18~60岁体检人群代谢综合征流行现状及影响因素分析[J]. 中国卫生统计, 2023, 40(5): 707-710. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGWT202305016.htmFEI L P, ZHOU Z X, ZHANG R, et al. To analyze the prevalence and influencing factors of metabolic syndrome in 18-60 years old physical examination population in Luzhou city[J]. Chinese Journal of Health Statistics, 2023, 40(5): 707-710. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGWT202305016.htm [4] 国家卫生计生委合理用药专家委员会, 中国药师协会. 冠心病合理用药指南(第2版)[J]. 中国医学前沿杂志(电子版), 2018, 10(6): 1-130. https://www.cnki.com.cn/Article/CJFDTOTAL-JRFS202106031.htmExpert Committee on Rational Drug Use, National Health and Family Planning Commission, Chinese Pharmacists Association. Guidelines for the rational use of drugs for coronary heart disease (2nd edition)[J]. Chinese Journal of the Frontiers of Medical Science (Electronic Version), 2018, 10(6): 1-130. https://www.cnki.com.cn/Article/CJFDTOTAL-JRFS202106031.htm [5] DOMMERMUTH R, EWING K. Metabolic syndrome: systems thinking in heart disease[J]. Prim Care, 2018, 45(1): 109-129. doi: 10.1016/j.pop.2017.10.003 [6] LAVIE C J, GERSH B J. Acute myocardial infarction: initial manifestations, management, and prognosis[J]. Mayo Clin Proc, 1990, 65(4): 531-548. doi: 10.1016/S0025-6196(12)60954-9 [7] THYGESEN K, ALPERT J S, JAFFE A S, et al. Fourth universal definition of myocardial infarction (2018)[J]. Glob Heart, 2018, 13(4): 305-338. doi: 10.1016/j.gheart.2018.08.004 [8] REYNOLDS H R, SHAW L J, MIN J K, et al. Outcomes in the ISCHEMIA trial based on coronary artery disease and ischemia severity[J]. Circulation, 2021, 144(13): 1024-1038. doi: 10.1161/CIRCULATIONAHA.120.049755 [9] 中华医学会糖尿病学分会. 中国2型糖尿病防治指南(2020年版)(下)[J]. 中国实用内科杂志, 2021, 41(9): 757-784. https://www.cnki.com.cn/Article/CJFDTOTAL-HLSJ202309001.htmDiabetes Society of Chinese Medical Association. Chinese Guidelines for the Prevention and Treatment of Type 2 diabetes(2020 Edition)(Ⅱ)[J]. Chinese Journal of Practical Internal Medicine, 2021, 41(9): 757-784. https://www.cnki.com.cn/Article/CJFDTOTAL-HLSJ202309001.htm [10] 中国高血压防治指南修订委员会, 高血压联盟(中国), 中华医学会心血管病学分会中国医师协会高血压专业委员会, 等. 中国高血压防治指南(2018年修订版)[J]. 中国心血管杂志, 2019, 24(1): 24-56. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGGZ201904005.htmChinese Committee for Revision of Guidelines for the Prevention and Treatment of Hypertension, Hypertension Alliance (China), Chinese Society of Cardiology, Chinese Medical Doctor Association, et al. 2018 Chinese guidelines for the management of hypertension[J]. Chinese Journal of Cardiovascular Medicine, 2019, 24(1): 24-56. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGGZ201904005.htm [11] 中华医学会糖尿病学分会. 中国2型糖尿病防治指南(2020年版)(上)[J]. 中国实用内科杂志, 2021, 41(8): 668-695. https://www.cnki.com.cn/Article/CJFDTOTAL-HBYX202112018.htmDiabetes Society of Chinese Medical Association. Guideline for the prevention and treatment of type 2 diabetes mellitus in China(2020 edition)(Part 1)[J]. Chinese Journal of Practical Internal Medicine, 2021, 41(8): 668-695. https://www.cnki.com.cn/Article/CJFDTOTAL-HBYX202112018.htm [12] 中华医学会心血管病学分会高血压学组, 中华心血管病杂志编辑委员会. 中国高血压患者血压血脂综合管理的专家共识[J]. 中华心血管病杂志, 2021, 49(6): 554-563.Hypertensive Group of Chinese Society of Cardiology of Chinese Medical Association. Expert consensus on the comprehensive management of blood pressure and dyslipidemia in Chinese hypertensive patients[J]. Chinese Journal of Cardiology, 2021, 49(6): 554-563. [13] WANG K Y, ZHENG Y Y, WU T T, et al. Predictive value of Gensini score in the long-term outcomes of patients with coronary artery disease who underwent PCI[J]. Front Cardiovasc Med, 2021, 8: 778615. DOI: 10.3389/fcvm.2021.778615. [14] 中国心血管健康与疾病报告编写组. 中国心血管健康与疾病报告2021概要[J]. 中国循环杂志, 2022, 37(6): 553-578. https://www.cnki.com.cn/Article/CJFDTOTAL-XFXZ202312019.htmThe Writing Committee of the Report on Cardiovascular Health and Diseases in China. Report on cardiovascular health and diseases in China 2021: an updated summary[J]. Chinese Circulation Journal, 2022, 37(6): 553-578. https://www.cnki.com.cn/Article/CJFDTOTAL-XFXZ202312019.htm [15] 李耀华, 谢萍. 代谢综合征与冠心病冠状动脉病变相关性分析[J]. 中国循证心血管医学杂志, 2017, 9(1): 41-45. https://www.cnki.com.cn/Article/CJFDTOTAL-PZXX201701013.htmLI Y H, XIE P. The correlation between metabolic syndrome and coronary artery lesions in patients with coronary heart disease[J]. Chinese Journal of Evidence-Based Cardiovascular Medicine, 2017, 9(1): 41-45. https://www.cnki.com.cn/Article/CJFDTOTAL-PZXX201701013.htm [16] 秦会敏, 程华. 多层螺旋CT评价腹型肥胖与冠心病Gensini评分的相关性[J]. 中国老年学杂志, 2020, 40(8): 1573-1577. https://www.cnki.com.cn/Article/CJFDTOTAL-ZLXZ202008003.htmQIN H M, CHENG H. The correlation between abdominal obesity and coronary heart disease Gensini score evaluated by multi-slice spiral CT[J]. Chinese Journal of Gerontology, 2020, 40(8): 1573-1577. https://www.cnki.com.cn/Article/CJFDTOTAL-ZLXZ202008003.htm [17] 郭明秋, 殷晓捷, 刁殿琰, 等. 脂质代谢水平与冠状动脉粥样硬化病变的关系[J]. 中国动脉硬化杂志, 2021, 29(2): 149-155. https://www.cnki.com.cn/Article/CJFDTOTAL-KDYZ202102010.htmGUO M Q, YIN X J, DIAO D Y, et al. Relationship between the levels of lipid metabolism and coronary atherosclerotic lesions[J]. Chinese Journal of Arteriosclerosis, 2021, 29(2): 149-155. https://www.cnki.com.cn/Article/CJFDTOTAL-KDYZ202102010.htm [18] 王欢欢, 贾斯达, 刘越, 等. 代谢综合征及其组分对冠状动脉介入术患者远期预后的影响[J]. 中华医学杂志, 2020, 100(21): 1623-1628.WANG H H, JIA S D, LIU Y, et al. The impact of metabolic syndrome and its individual components on long-term prognosis of patients undergoing percutaneous coronary intervention[J]. National Medical Journal of China, 2020, 100(21): 1623-1628. [19] 师瑞, 冯磊, 唐灵通, 等. 糖尿病患者血糖波动评价指标研究进展[J]. 中华全科医学, 2022, 20(12): 2105-2109. doi: 10.16766/j.cnki.issn.1674-4152.002780SHI R, FENG L, TANG L T, et al. Research progress on evaluation indicators of blood glucose fluctuation in patients with diabetes[J]. Chinese Journal of General Practice, 2022, 20(12): 2105-2109. doi: 10.16766/j.cnki.issn.1674-4152.002780 [20] 赵茂宇, 李佑美, 刘焕云, 等. 胰岛素抵抗标志物在动脉粥样硬化发病中的研究进展[J]. 基础医学与临床, 2022, 42(8): 1302-1305. https://www.cnki.com.cn/Article/CJFDTOTAL-JCYL202208027.htmZHAO M Y, LI Y M, LIU H Y, et al. Research progress of insulin resistance markers in atherogenesis[J]. Basic and Clinical Medicine, 2022, 42(8): 1302-1305. https://www.cnki.com.cn/Article/CJFDTOTAL-JCYL202208027.htm [21] SALTIEL A R, OLEFSKY J M. Inflammatory mechanisms linking obesity and metabolic disease[J]. J Clin Invest, 2017, 127(1): 21-24. [22] KUNZ H E, HART C R, GRIES K J, et al. Adipose tissue macrophage populations and inflammation are associated with systemic inflammation and insulin resistance in obesity[J]. Am J Physiol Endocrinol Metab, 2021, 321(1): E105-E121. doi: 10.1152/ajpendo.00070.2021 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 1223
- HTML全文浏览量: 602
- PDF下载量: 23
- 被引次数: 0
