

sTREM-1 and MMP-9 in predicting futile recanalization after endovascular treatment in acute middle cerebral artery occlusion ischemic stroke
-
摘要:
目的 分析急性大脑中动脉闭塞脑卒中(MCAO-AIS)患者机械取栓术后无效再通的影响因素,探讨血清可溶性髓样细胞触发受体-1(sTREM-1)及基质金属蛋白酶-9(MMP-9)水平对无效再通的预测价值。 方法 前瞻性纳入2020年8月—2022年9月在中国科学技术大学附属第一医院神经内科行机械取栓并实现再通的115例MCAO-AIS患者。根据术后3个月改良Rankin量表(mRS)评分分为有效再通组(45例)和无效再通组(70例)。采用多因素logistic回归分析探究无效再通的独立影响因素,绘制ROC曲线评估sTREM-1、MMP-9水平对无效再通的预测价值。 结果 与有效再通组比较,无效再通组患者年龄、入院时美国国立卫生研究院卒中量表(NIHSS)评分、血糖、中性粒细胞与淋巴细胞比值、血清sTREM-1及MMP-9水平较高,术前Alberta脑卒中计划早期计算机断层扫描评分(ASPECTs)较低(P < 0.05)。多因素logistic回归分析显示,年龄(OR=1.060,P=0.030,95% CI:1.006~1.117)、MMP-9水平(OR=1.007,P=0.019,95% CI:1.001~1.014)、sTREM-1水平(OR=1.009,P < 0.001,95% CI:1.004~1.014)是患者术后无效再通的独立影响因素。sTREM-1、MMP-9预测无效再通的AUC分别为0.837、0.763。 结论 年龄、血清sTREM-1及MMP-9水平是MCAO-AIS患者术后无效再通的独立影响因素;sTREM-1及MMP-9是预测无效再通的潜在生物标志物。 -
关键词:
- 急性大脑中动脉闭塞脑卒中 /
- 机械取栓 /
- 可溶性髓样细胞触发受体-1 /
- 基质金属蛋白酶-9 /
- 无效再通
Abstract:Objective To analyze the influencing factors of futile recanalization after endovascular thrombectomy (EVT) in patients with acute middle cerebral artery occlusion stroke (MCAO-AIS), and to explore the predictive value of serum sTREM-1 and MMP-9 levels for futile recanalization. Methods A total of 115 MCAO-AIS patients who underwent EVT and achieved successful recanalization in the Department of Neurology, the First Affiliated Hospital of University of Science and Technology of China (USTC) from August 2020 to September 2022, were prospectively enrolled. The patients were divided into the meaningful recanalization and futile recanalization groups according to the mRS score 3 months after EVT. Independent influencing factors for futile recanalization were analyzed by multivariate logistic regression. The receiver operating characteristic curve was used to analyze the efficacy of sTREM-1 and MMP-9 in predicting futile recanalization. Results Compared with the meaningful recanalization group, the futile recanalization group had higher age, NIHSS score at admission, blood glucose, neutrophil-to-lymphocyte ratio, serum sTREM-1 and MMP-9 levels, and lower preoperative ASPECT score (P < 0.05). Multivariate logistic regression analysis showed that age (OR=1.060, P=0.030, 95% CI: 1.006-1.117), serum MMP-9 level (OR=1.007, P=0.019, 95% CI: 1.001-1.014), and serum sTREM-1 level (OR=1.009, P < 0.001, 95% CI: 1.004-1.014) were independent influencing factors for post-procedural futile recanalization. The AUC of sTREM-1 and MMP-9 for predicting futile recanalization were 0.837 and 0.763, respectively. Conclusion Age, serum sTREM-1 and MMP-9 level are independent influencing factors for futile recanalization in MCAO-AIS patients after EVT. sTREM-1 and MMP-9 are potential biomarkers for predicting futile recanalization. -

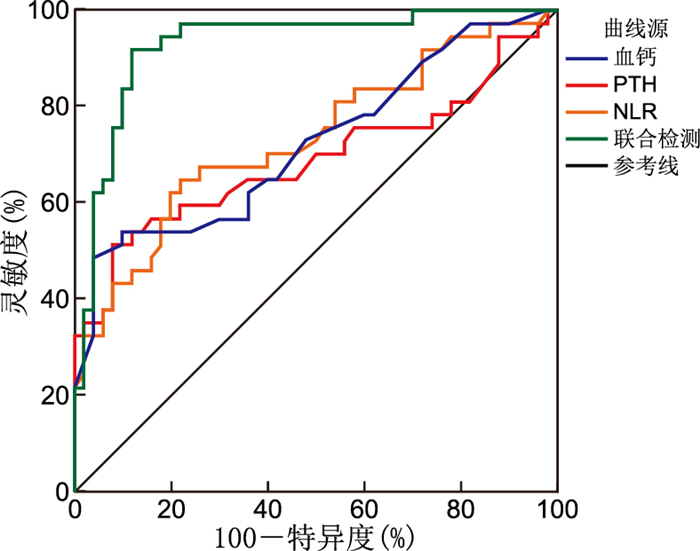
图 1 血清sTREM-1、MMP-9水平以及两指标联合预测MCAO-AIS患者EVT后无效再通的ROC曲线
Figure 1. ROC curves of serum sTREM-1, MMP-9, and their combination for predicting futile recanalization
表 1 有效再通组与无效再通组MCAO-AIS患者基线资料比较
Table 1. Comparison of baseline characteristics between MCAO-AIS patients in the meaningful recanalization group and the futile recanalization group
组别 例数 年龄
(x±s,岁)性别
(男性/女性,例)高血压
[例(%)]糖尿病
[例(%)]冠心病
[例(%)]心房颤动
[例(%)]既往脑卒中/TIA[例(%)] 吸烟史
[例(%)]饮酒史
[例(%)]静脉溶栓
[例(%)]有效再通组 45 62.60±13.32 25/20 27(60.0) 3(6.7) 8(17.8) 10(22.2) 2(4.4) 8(17.8) 6(13.3) 17(37.8) 无效再通组 70 70.21±11.34 33/37 37(52.9) 13(18.6) 6(8.6) 19(27.1) 11(15.7) 8(11.4) 8(11.4) 27(38.6) 统计量 3.280a 0.775b 0.566b 3.241b 2.171b 0.352b 3.470b 0.922b 0.093b 0.007b P值 0.001 0.379 0.452 0.072 0.141 0.553 0.063 0.337 0.760 0.932 组别 例数 收缩压
(x±s,mmHg)舒张压
(x±s,mmHg)入院时ASPECTs评分
[M(P25, P75), 分]入院时NIHSS评分
[M(P25, P75), 分]穿刺至再通时间
[M(P25, P75),min]脑卒中类型[例(%)] 大动脉粥样硬化型 心源性栓塞型 其他类型 有效再通组 45 145.11±18.36 84.93±13.02 10(9, 10) 14.00(10.50, 17.00) 65.0(50.0, 85.0) 23(51.1) 19(42.2) 3(6.7) 无效再通组 70 147.27±23.29 84.16±12.83 9(8, 10) 18.00(12.75, 20.00) 70.0(52.5, 90.0) 31(44.3) 35(50.0) 4(5.7) 统计量 0.526a 0.315a -3.637c -2.888c -0.795c 0.599c P值 0.600 0.753 <0.001 0.004 0.427 0.549 注:a为t值,b为χ2值,c为Z值;1 mmHg=0.133 kPa。  下载: 导出CSV
下载: 导出CSV
表 2 2组MCAO-AIS患者sTREM-1水平及其他实验室指标比较
Table 2. Comparison of sTREM-1 levels and other laboratory indicators between the two groups of MCAO-AIS patients
组别 例数 胱抑素C
[M(P25, P75), mg/L]D-二聚体
[M(P25, P75), mg/L]血糖
[M(P25, P75), mmol/L]白细胞
(x±s,×109/L)中性粒细胞
(x±s,×109/L)有效再通组 45 0.92(0.78, 1.11) 0.79(0.40, 2.34) 6.60(5.85, 8.24) 8.33±2.34 6.66±2.30 无效再通组 70 0.93(0.81, 1.10) 1.42(0.73, 2.54) 7.90(6.45, 9.25) 8.71±3.17 7.16±3.19 统计量 -0.109a -1.848a -2.378a 0.753b 0.977b P值 0.913 0.065 0.017 0.453 0.331 组别 例数 单核细胞
[M(P25, P75), 109/L]淋巴细胞
(x±s,109/L)NLR
(x±s)MMP-9
[M(P25, P75), ng/mL]sTREM-1
[M(P25, P75), pg/L]有效再通组 45 0.36(0.28, 0.52) 1.18±0.51 7.14±4.60 149.96(107.59, 194.57) 232.03(185.59, 295.05) 无效再通组 70 0.35(0.19, 0.56) 1.10±0.68 9.26±6.14 250.84(157.20, 394.12) 389.91(279.26, 579.16) 统计量 -0.694a 0.713b 2.116b -4.742a -6.089a P值 0.488 0.477 0.037 <0.001 <0.001 注:a为Z值,b为t值。
下载: 导出CSV
表 3 MCAO-AIS患者术后无效再通影响因素的多因素logistic回归分析
Table 3. Multivariate logistic regression analysis of futile recanalization in MCAO-AIS patients
变量 B SE Waldχ2 P值 OR值 95% CI 年龄 0.058 0.027 4.696 0.030 1.060 1.006~1.117 糖尿病 0.441 1.045 0.178 0.673 1.554 0.200~12.053 既往脑卒中/TIA 1.820 0.969 3.527 0.060 6.173 0.924~41.263 ASPECTs评分 -0.267 0.234 1.301 0.254 0.766 0.484~1.211 入院时NIHSS评分 0.054 0.058 0.868 0.351 1.056 0.942~1.183 血糖 -0.168 0.120 1.979 0.159 0.845 0.669~1.068 D-二聚体 0.088 0.074 1.428 0.232 1.092 0.945~1.261 NLR 0.017 0.056 0.088 0.766 1.017 0.911~1.136 MMP-9 0.007 0.003 5.500 0.019 1.007 1.001~1.014 sTREM-1 0.009 0.002 12.722 <0.001 1.009 1.004~1.014
下载: 导出CSV
表 4 sTREM-1、MMP-9水平预测MCAO-AIS患者EVT后无效再通影响因素的预测价值
Table 4. ROC curve analysis of serum sTREM-1 and MMP-9 levels for predicting futile recanalization
项目 AUC(95% CI) P值 最佳截
断值灵敏度
(%)特异度
(%)sTREM-1(pg/mL) 0.837(0.764~0.910) <0.001 346.97 67.1 91.1 MMP-9(ng/mL) 0.763(0.676~0.849) <0.001 243.39 52.9 93.3 sTREM-1+MMP-9 0.866(0.798~0.933) <0.001 84.3 77.8
下载: 导出CSV
-
[1] XU X J, YANG K, XU J F, et al. Endovascular treatment in patients with middle cerebral artery occlusion of different aetiologies[J]. Neuroradiology, 2023, 65(3): 609-618. doi: 10.1007/s00234-022-03078-6 [2] MAKKAWI S, BUKHARI J I, SALAMATULLAH H K, et al. Endovascular thrombectomy after anterior circulation large vessel ischemic stroke: an updated meta-analysis[J]. Syst Rev, 2024, 13(1): 255. DOI: 10.1186/s13643-024-02670-6. [3] 中国卒中学会, 中国卒中学会神经介入分会, 中华预防医学会卒中预防与控制专业委员会介入学组, 等. 急性缺血性卒中血管内治疗中国指南2023[J]. 中国卒中杂志, 2023, 18(6): 684-711.Chinese Stroke Association, Chinese Interventional Neuroradiology Society, Intervention Group of Committee of Stroke Prevention and Control of Chinese Preventive Medicine Association, et al. Chinese guideline for endovascular treatment of acute ischemic stroke 2023[J]. Chinese Journal of Stroke, 2023, 18(6): 684-711. [4] 邓刚, 秦川, 田代实. 急性缺血性脑卒中血管内治疗无效再通的病理生理机制和潜在治疗策略[J]. 中华神经科杂志, 2022, 55(12): 1423-1430.DENG G, QIN C, TIAN D L. Pathophysiological mechanisms of futile recanalization following endovascular therapy for acute ischemic stroke due to large vessel occlusion and potential targeted therapeutic strategy[J]. Chinese Journal of Neurology, 2022, 55(12): 1423-1430. [5] ZHANG C Y, KAN X G, ZHANG B L, et al. The role of triggering receptor expressed on myeloid cells-1 (TREM-1) in central nervous system diseases[J]. Mol Brain, 2022, 15(1): 84. DOI: 10.1186/s13041-022-00969-w. [6] SISKIND S, BRENNER M, WANG P. TREM-1 modulation strategies for sepsis[J]. Front Immunol, 2022, 13: 907387. DOI: 10.3389/fimmu.2022.907387. [7] 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国急性缺血性脑卒中诊治指南2018[J]. 中华神经科杂志, 2018, 51(9): 666-682.Chinese Society of Neurology, Chinese Stroke Society. Chinese guidelines for diagnosis and treatment of acute ischemic stroke 2018[J]. Chinese Journal of Neurology, 2018, 51(9): 666-682. [8] ZHOU T F, YI T Y, LI T X, et al. Predictors of futile recanalization in patients undergoing endovascular treatment in the DIRECT-MT trial[J]. J Neurointerv Surg, 2022, 14(8): 752-755. doi: 10.1136/neurintsurg-2021-017765 [9] DENG G, XIAO J, YU H H, et al. Predictors of futile recanalization after endovascular treatment in acute ischemic stroke: a meta-analysis[J]. J Neurointerv Surg, 2022, 14(9): 881-885. doi: 10.1136/neurintsurg-2021-017963 [10] 李瑞, 郭玲玲, 王黎, 等. 急性缺血性脑卒中患者机械取栓的预后因素分析[J]. 中华全科医学, 2020, 18(9): 1455-1457.LI R, GUO L L, WANG L, et al. Analysis of prognostic factors of mechanical thrombectomy in acute ischemic stroke patients[J]. Chinese Journal of General Practice, 2020, 18(9): 1455-1457. [11] SU M X, ZHOU Y, CHEN Z L, et al. Cystatin C predicts futile recanalization in patients with acute ischemic stroke after endovascular treatment[J]. J Neurol, 2022, 269(2): 966-972. doi: 10.1007/s00415-021-10680-w [12] ZHAO M, DAI Z Z, LIU R, et al. Post-procedural plasma D-dimer level may predict futile recanalization in stroke patients with endovascular treatment[J]. J Stroke Cerebrovasc Dis, 2025, 34(5): 108248. DOI: 10.1016/j.jstrokecerebrovasdis.2025.108248. [13] ZANG N L, LIN Z Z, HUANG K B, et al. Biomarkers of unfavorable outcome in acute ischemic stroke patients with successful recanalization by endovascular thrombectomy[J]. Cerebrovasc Dis, 2020, 49(6): 583-592. doi: 10.1159/000510804 [14] 杜仁峰, 余波, 潘丹红, 等. 缺血性脑卒中血脑屏障受损及修复的神经炎性机制研究进展[J]. 华西医学, 2022, 37(4): 622-626.DU R F, YU B, PAN D H, et al. Research progress on neuroinflammatory mechanisms of blood-brain barrier damage and repair in ischemic stroke[J]. West China Medical Journal, 2022, 37(4): 622-626. [15] ARKELIUS K, WENDT T S, ANDERSSON H, et al. LOX-1 and MMP-9 inhibition attenuates the detrimental effects of delayed rt-PA therapy and improves outcomes after acute ischemic stroke[J]. Circ Res, 2024, 134(8): 954-969. doi: 10.1161/CIRCRESAHA.123.323371 [16] KOLLIKOWSKI A M, PHAM M, MÄRZ A G, et al. MMP-9 release into collateral blood vessels before endovascular thrombectomy to assess the risk of major intracerebral haemorrhages and poor outcome for acute ischaemic stroke: a proof-of-concept study[J]. EBioMedicine, 2024, 103: 105095. DOI: 10.1016/j.ebiom.2024.105095. [17] 林巧茂, 李阔, 项宁, 等. 血清可溶性髓系细胞触发受体-1与老年急性缺血性脑卒中严重程度及预后的关系[J]. 实用老年医学, 2022, 36(8): 827-832.LIN Q M, LI K, XIANG L, et al. Relationship between serum soluble triggering receptor expressed on myeloid cells-1 and the severity and prognosis of elderly patients with acute ischemic stroke[J]. Practical Geriatrics, 2022, 36(8): 827-832. [18] CHEN Z, YI X, FU W, et al. Higher soluble TREM-1 levels are associated with cognitive impairment after acute ischemic stroke[J]. Front Aging Neurosci, 2024, 16: 1463065. DOI: 10.3389/fnagi.2024.1463065. [19] WU X Y, ZENG H H, XU C R, et al. TREM1 regulates neuroinflammatory injury by modulate proinflammatory subtype transition of microglia and formation of neutrophil extracellular traps via interaction with SYK in experimental subarachnoid hemorrhage[J]. Front Immunol, 2021, 12: 766178. DOI: 10.3389/fimmu.2021.766178. [20] XIE Y L, HE W, MA L, et al. Endothelial TREM-1 receptor regulates the blood-brain barrier integrity after intracerebral hemorrhage in mice via SYK/β-catenin signaling[J]. CNS Neurosci Ther, 2023, 29(11): 3228-3238. doi: 10.1111/cns.14255 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 2
- HTML全文浏览量: 2
- PDF下载量: 0
- 被引次数: 0
