

The application of KELIM score and CRS score in patients with advanced epithelial ovarian cancer undergoing neoadjurant chemotherapy
-
摘要:
目的 探讨CA-125消除速率常数K(KELIM)及化疗反应评分(CRS)对晚期上皮性卵巢癌(AEOC)患者预后的预测价值, 同时探讨KELIM评分和CRS评分与乳腺癌易感基因(BRCA)之间的相关性。 方法 收集2014年11月—2023年5月在蚌埠医科大学第一附属医院接受中间型肿瘤细胞减灭术的83例Ⅲ~Ⅳ期AEOC患者的BRCA基因状态、KELIM评分、CRS评分及随访资料。将BRCA基因分为突变型、野生型;将KELIM分为KELIM≥1、KELIM<1;将CRS分为CRS3、CRS1+2,通过χ2检验分析BRCA状态与KELIM评分、CRS评分的相关性, log-rank检验和多变量Cox回归模型评估其与无进展生存期(PFS)、总生存期(OS)的关系。 结果 83例AEOC患者中BRCA突变组20例(24.1%),野生组63例(75.9%)。BRCA突变组KELIM≥1、CRS3比例高于野生组(P<0.05)。Cox多变量分析显示,BRCA基因、FIGO分期、R0减瘤是AEOC患者PFS的独立影响因素(P<0.05),BRCA基因、CRS评分、KELIM评分、R0减瘤是AEOC患者OS的独立影响因素(P<0.05)。 结论 CRS评分、KELIM评分可作为AEOC患者预后有价值的预测指标;BRCA突变状态与CRS3及KELIM≥1均呈显著正相关,提示其可作为AEOC患者化疗反应的良好预测指标。 -
关键词:
- 卵巢癌 /
- 新辅助化疗 /
- 化疗反应评分 /
- CA125消除速率常数K /
- 乳腺癌易感基因
Abstract:Objective To explore the prognostic value of the CA-125 elimination rate constant K (KELIM) and the chemotherapy response score (CRS) in patients with advanced epithelial ovarian cancer (AEOC), and to investigate the correlation between KELIM score, CRS score, and breast cancer susceptibility gene (BRCA) status. Methods Clinical data, including BRCA gene status, KELIM score, CRS score, and follow-up outcomes, were retrospectively collected from 83 patients with stage Ⅲ-Ⅳ AEOC who underwent intermediate cytoreductive surgery at the First Affiliated Hospital of Bengbu Medical University from November 2014 to May 2023. BRCA genes were classified as mutant type or wild type, KELIM was classified as ≥ 1 or < 1, CRS was classified as CRS3 or CRS1+2. Chi-square test was used to analyze the correlation between BRCA status and KELIM and CRS scores. The log-rank test and multivariate Cox regression model were used to evaluate their relationship with progression-free survival (PFS) and overall survival (OS). Results Among the 83 AEOC patients, 20 cases (24.1%) were in the BRCA mutant group while 63 cases (75.9%) were in the wild type group. In the BRCA mutant group, the proportions of KELIM ≥ 1 and CRS3 were higher than those in the wild type group (P < 0.05). Multivariate Cox analysis identified BRCA gene, FIGO stage, and R0 cytoreduction as independent predictors of PFS in AEOC patients (P < 0.05), while BRCA gene, CRS score, KELIM score, and R0 cytoreduction were independent predictors of OS in AEOC patients (P < 0.05). Conclusion Both the CRS and KELIM scores are valuable predictive indicators for the prognosis in AEOC patients. The BRCA mutation status was significantly positively correlated with both CRS3 and KELIM ≥ 1, suggesting that it can serve as a good predictor of chemotherapy response in AEOC patients. -

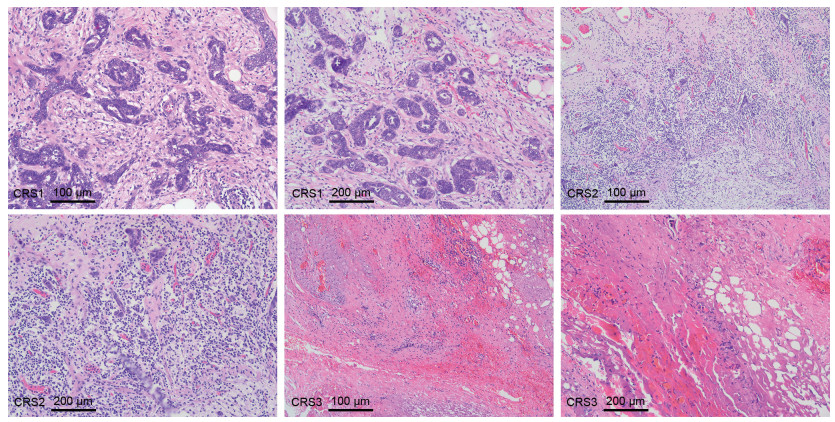
图 1 晚期浆液性卵巢癌患者大网膜组织的CRS评分
Figure 1. CRS score of omental tissue in patients with advanced serous ovarian cancer

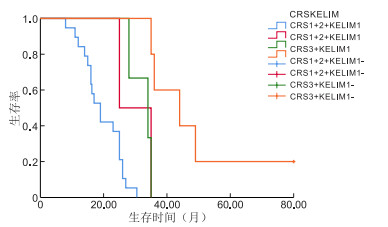
图 2 晚期上皮性卵巢癌患者PFS的生存曲线
Figure 2. Survival curves of PFS for patients with advanced epithelial ovarian cancer

图 3 晚期上皮性卵巢癌患者OS的生存曲线
Figure 3. Survival curves of OS for patients with advanced epithelial ovarian cancer
表 1 卵巢高级别浆液性癌化疗反应评分标准
Table 1. Scoring criteria for chemotherapy response in high-grade serous ovarian cancer
化疗反应评分 要点 肿瘤 间质退行性纤维炎性改变 CRS1 无或轻微的肿瘤反应 主导 无或轻微 CRS2 部分肿瘤反应 分布规律,多灶易识别 明显,多灶或弥漫 CRS3 完全或接近完全的肿瘤反应 无、单个或小灶(≤2 mm) 主导,极少数情况下无  下载: 导出CSV
下载: 导出CSV
表 2 2组晚期上皮性卵巢癌患者临床特征比较[例(%)]
Table 2. Comparison of clinical characteristics of two groups of patients with advanced epithelial ovarian cancer[cases(%)]
项目 BRCA野生型(n=63) BRCA突变型(n=20) 统计量 P值 年龄(x±s,岁) 59.83±9.36 55.85±10.23 1.619a 0.109 FIGO分期 0.673d Ⅲ期 56(88.9) 19(95.0) Ⅳ期 7(11.1) 1(5.0) 病理分级[例(%)] -1.349b 0.177 Ⅰ级 8(12.7) 1(5.0) Ⅱ级 12(19.0) 2(10.0) Ⅲ级 43(68.3) 17(85.0) 是否满意减瘤[例(%)] 0.490c 0.587 R0 43(68.2) 15(75.0) 非R0 20(31.7) 5(25.0) 化疗反应评分[例(%)] 15.230c <0.001 CRS1 21(33.3) 3(15.0) CRS2 30(47.6) 4(20.0) CRS3 12(19.0) 13(65.0) KELIM值[例(%)] 11.176c 0.002 KELIM<1 50(79.4) 8(40.0) KELIM≥1 13(20.6) 12(60.0) 新辅助化疗方案[例(%)] 0.191d 紫杉醇+铂类 49(77.8) 14(70.0) 紫杉醇+铂类+贝伐 1(1.6) 0 化疗+腹腔化疗 5(7.9) 5(25.0) 其他 8(12.7) 1(5.0) PARPi[例(%)] 0.096c 0.757 应用 29(46.0) 10(50.0) 未应用 34(54.0) 10(50.0) 注:a为t值,b为Z值,c为χ2值,d为采用Fisher精确检验。
下载: 导出CSV
表 3 AEOC患者BRCA基因状态与CRS评分、KELIM评分分组的关系比较[例(%)]
Table 3. Comparison of the relationship between BRCA mutation status and CRS/KELIM score groups in patients with AEOC[cases(%)]
项目 CRS评分 野生组 突变组 χ2值 P值 KELIM评分 野生组 突变组 χ2值 P值 BRCA1/2 CRS1+2 51(81.0) 7(35.0) 15.230 <0.001 KELIM<1 50(79.4) 8(40.0) 11.176 0.002 CRS3 12(19.0) 13(65.0) KELIM≥1 13(20.6) 12(60.0) BRCA1 CRS1+2 51(76.1) 7(43.8) 4.984 0.026 KELIM<1 50(74.6) 8(50.0) 2.643 0.104 CRS3 16(23.9) 9(56.2) KELIM≥1 17(25.4) 8(50.0) BRCA2 CRS1+2 58(73.4) 0 6.574 0.010 KELIM<1 58(73.4) 0 6.574 0.010 CRS3 21(26.6) 4(100.0) KELIM≥1 21(26.6) 4(100.0)
下载: 导出CSV
表 4 晚期上皮性卵巢癌PFS、OS单因素分析
Table 4. Univariate analysis of PFS and OS in advanced epithelial ovarian cancer
项目 PFS OS 中位数(月) log-rankχ2值 P值 中位数(月) log-rankχ2值 P值 FIGO分期 13.181 <0.001 5.098 0.024 Ⅲ期 19.50 26.00 Ⅳ期 11.00 16.00 病理分级 0.128 0.938 3.787 0.151 Ⅰ级 15.00 30.50 Ⅱ级 13.00 16.00 Ⅲ级 18.00 25.00 是否满意减瘤 5.768 0.016 9.269 0.002 R0 21.00 28.00 非R0 15.00 16.30 化疗反应评分 4.638 0.031 17.017 <0.001 CRS1+2 17.00 19.00 CRS3 23.00 35.00 KELIM值 6.589 0.010 14.299 <0.001 KELIM<1 17.60 19.00 KELIM≥1 30.00 36.00 CRS+KELIM 7.789 0.051 23.394 <0.001 CRS3+KELIM≥1 32.00 44.00 CRS3+KELIM<1 17.90 34.00 CRS1+2+KELIM≥1 17.00 25.00 CRS1+2+KELIM<1 17.00 19.00 BRCA状态 14.160 <0.001 10.301 0.001 野生型 16.00 23.00 突变型 32.00 44.00 新辅助化疗方案 0.653 0.721 0.216 0.898 紫杉醇+铂类 17.90 25.00 紫杉醇+铂类+贝伐 - - 化疗+腹腔化疗 18.00 - 其他 19.50 - 是否应用PARPi 1.777 0.183 0.497 0.418 应用 17.90 25.00 未应用 18.00 25.00 注:-表示该组数据未达到中位数。
下载: 导出CSV
表 5 晚期上皮性卵巢癌PFS、OS多因素分析
Table 5. Multivariate analysis of PFS and OS in advanced epithelial ovarian cancer
变量 PFS OS HR(95% CI) P值 HR(95% CI) P值 BRCA基因状态 4.687(1.777~12.357) 0.002 16.345(2.531~105.563) 0.003 CRS评分 0.686(0.297~1.587) 0.378 5.322(1.114~25.430) 0.036 KELIM评分 0.995(0.426~2.324) 0.990 27.212(2.313~320.171) 0.009 FIGO分期 0.273(0.103~0.721) 0.009 0.823(0.283~2.393) 0.720 是否满意减瘤 2.154(1.129~4.111) 0.020 2.873(1.025~8.055) 0.045
下载: 导出CSV
-
[1] SPILIOTIS J, IAVAZZO C, FOTIOU A, et al. Upfront or intermediate treatment of advanced ovarian cancer patients with cytoreduction plus HIPEC: results of a retrospective study[J]. J Surg Oncol, 2021, 123(2): 630-637. doi: 10.1002/jso.26280 [2] 陈川, 张天骄, 李敏, 等. 初次肿瘤细胞减灭术与中间性肿瘤细胞减灭术对晚期卵巢癌患者远期生存的影响真实世界临床研究[J]. 现代生物医学进展, 2023, 23(24): 4673-4677.CHEN C, ZHANG T J, LI M, et al. Real-world clinical study on the impact of primary tumor cell reduction and intermediate tumor cell reduction on the long-term survival of patients with advanced ovarian cancer[J]. Modern Biomedical Progress, 2023, 23(24): 4673-4677. [3] 刘格格, 王丽华, 李燕华. 上皮性卵巢癌患者的BRCA1/2基因状态与其临床病理特征的相关性分析[J]. 中华全科医学, 2023, 21(5): 749-752, 768. doi: 10.16766/j.cnki.issn.1674-4152.002974LIU G G, WANG L H, LI Y H. Correlation analysis of BRCA1/2 gene status and its clinical pathological characteristics in patients with epithelial ovarian cancer[J]. Chinese Journal of General Practice, 2023, 21(5): 749-752, 768. doi: 10.16766/j.cnki.issn.1674-4152.002974 [4] MARCHETTI C, ATASEVEN B, PERRONE A M, et al. Clinical characteristics and survival outcome of early-stage, high-grade, serous tubo-ovarian carcinoma according to BRCA mutational status[J]. Gynecol Oncol, 2024, 187: 170-177. doi: 10.1016/j.ygyno.2024.05.008 [5] RODOLAKIS I, PERGIALIOTIS V, LIONTOS M, et al. Chemotherapy response score in ovarian cancer patients: an overview of its clinical utility[J]. J Clin Med, 2023, 12(6): 2155. DOI: 10.3390/jcm12062155. [6] LIONTOS M, ANDRIKOPOULOU A, KOUTSOUKOS K, et al. Neutrophil-to-lymphocyte ratio and chemotherapy response score as prognostic markers in ovarian cancer patients treated with neoadjuvant chemotherapy[J]. J Ovarian Res, 2021, 14(1): 148. DOI: 10.1186/s13048-021-00902-0. [7] LI C, CUI Q L, WANG X H, et al. CA-125 elimination rate constant K (KELIM) as a promising predictor of complete cytoreduction after neoadjuvant chemotherapy in advanced ovarian cancer patients: a retrospective study from two Chinese hospitals[J]. BMC Cancer, 2024, 24(1): 609. DOI: 10.1186/s12885-024-12252-3. [8] KUS F, GUVEN D C, YILDIRIM H C, et al. KELIM score predicts outcome in patients with platinum-resistant/refractory recurrent ovarian cancer[J]. Biomark Med, 2023, 17(7): 379-389. doi: 10.2217/bmm-2022-0923 [9] YOU B, ROBELIN P, TOD M, et al. CA-125 ELIMination rate constant K (KELIM) is a marker of chemosensitivity in patients with ovarian cancer: results from the Phase Ⅱ CHIVA trial[J]. Clin Cancer Res, 2020, 26(17): 4625-4632. doi: 10.1158/1078-0432.CCR-20-0054 [10] BÖHM S, FARUQI A, SAID I, et al. Chemotherapy response score: development and validation of a system to quantify histopathologic response to neoadjuvant chemotherapy in tubo-ovarian high-grade serous carcinoma[J]. J Clin Oncol, 2015, 33(22): 2457-2463. doi: 10.1200/JCO.2014.60.5212 [11] 王少明, 郑荣寿, 韩冰峰, 等. 2022年中国人群恶性肿瘤发病与死亡年龄特征分析[J]. 中国肿瘤, 2024, 33(3): 165-174.WANG S M, ZHENG R S, HAN B F, et al. Analysis of the age of incidence and death of malignant tumors in the Chinese population in 2022[J]. Chinese Tumors, 2024, 33(3): 165-174. [12] 倪孟冬, 吴小华. 晚期卵巢癌新辅助化疗联合间歇性肿瘤细胞减灭术[J]. 中国实用妇科与产科杂志, 2023, 39(7): 701-706.NI M D, WU X H. New adjuvant chemotherapy combined with intermittent tumor cell reduction for advanced ovarian cancer[J]. Chinese Journal of Practical Gynecology and Obstetrics, 2023, 39(7): 701-706. [13] 程晓东, 王芬芬. 复发性卵巢癌的诊治热点[J]. 浙江医学, 2021, 43(15): 1593-1599.CHENG X D, WANG F F. Diagnosis and treatment of recurrent ovarian cancer[J]. Zhejiang Medicine, 2021, 43(15): 1593-1599. [14] PIGNATA S, OZA A, HALL G, et al. Overall survival with maintenance olaparib in platinum-sensitive relapsed ovarian cancer by somatic or germline BRCA and homologous recombination repair mutation status[J]. Br J Cancer, 2025, 132(8): 725-732. doi: 10.1038/s41416-025-02966-x [15] PIEDIMONTE S, MURRAY C, ATENAFU EG, et al. Correlating the KELIM (CA125 elimination rate constant K) score and the chemo-response score as predictors of chemosensitivity in patients with advanced ovarian carcinoma[J]. Gynecol Oncol, 2024, 187: 92-97. doi: 10.1016/j.ygyno.2024.04.009 -


 点击查看大图
点击查看大图
计量
- 文章访问数: 15
- HTML全文浏览量: 7
- PDF下载量: 1
- 被引次数: 0
