

Heterogeneous frailty trajectory and prognostic analysis in elderly gastric cancer survivors
-
摘要:
目的 探讨老年胃癌幸存者虚弱症异质性变化轨迹及影响因素,并进行预后分析。 方法 选取2020年6月—2022年6月江苏大学附属医院收治的488例老年胃癌患者,采用Tilburg虚弱指数(TFI)评估患者入院时和术后1、3、6、9、12个月时的虚弱程度。采用增长混合模型(GMM)识别虚弱轨迹亚型,并采用多因素logistic回归分析研究不同轨迹亚型的影响因素,采用Kaplan-Meier生存曲线分析不同轨迹亚型与患者总体生存率的关系。 结果 GMM模型识别出3种虚弱轨迹亚型,分别为低程度虚弱下降型[252例(51.6%)]、中程度虚弱平稳型[124例(25.4%)]和中程度虚弱增长型[112例(23.0%)]。多因素logistic回归分析显示,年龄、糖尿病、贫血、婚姻状况、个人月收入和微型营养评估量表(MNA-SF)评分均为中程度虚弱平稳型的独立影响因素(P<0.05);年龄、糖尿病、家庭照顾者、个人月收入、MNS-SF评分和社会支持评定量表(SSRS)评分均为中程度虚弱增长型的独立影响因素(P<0.05)。低程度虚弱下降型总体生存率高于中程度虚弱平稳型和中程度虚弱增长型(P<0.05);中程度虚弱平稳型总体生存率高于中程度虚弱增长型(P<0.05)。 结论 老年胃癌幸存者术后表现出3种虚弱轨迹亚型,不同虚弱轨迹亚型有不同的独立影响因素且和预后相关。 Abstract:Objective To explore the heterogeneous frailty trajectories among older survivors of gastric cancer and to examine their influencing factors and prognostic significance. Methods A total of 488 elderly gastric cancer patients admitted to our hospital between June 2020 and June 2022 were selected. Patients ' frailty was assessed by Tilburg frailty indicator (TFI) at hospital admission and at 1, 3, 6, 9, and 12 months after surgery. Growth mixture modeling (GMM) was used to identify distinct frailty trajectory subtypes. Multifactorial logistic regression was used to analyze the factors associated with different frailty trajectory subtypes. Kaplan-Meier survival curves were used to analyze the relationship between different frailty trajectory subtypes and overall patient survival. Results The GMM model identified three subtypes of frailty trajectories: 252 cases (51.6%) of low-degree declining frailty, 124 cases (25.4%) of medium-degree stable frailty, and 112 cases (23.0%) of medium-degree increasing frailty. Multivariate logistic regression analysis showed that age, diabetes, anemia, marital status, individual monthly income, and mini-nutritional assessment short-form (MNS-SF) score were independent predictors of moderate-degree stable frailty (P < 0.05). Age, diabetes, family caregiver, individual monthly income, MNS-SF score, and social support rating scale (SSRS) score were independently associated with the moderate-degree increasing frailty (P < 0.05). Overall survival rate was higher in the low-degree declining frailty than that in the moderate-degree stable frailty and moderate-degree increasing frailty (P < 0.05). Overall survival was higher in the moderate-degree stable frailty than that in the moderate-degree increasing frailty (P < 0.05). Conclusion Elderly gastric cancer survivors exhibit three frailty trajectory subtypes after surgery. These trajectory subtypes are influenced by different clinical and social factors and are closely associated with prognosis. -
Key words:
- Gastric cancer /
- Frailty /
- Older age /
- Trajectory /
- Predictors
-

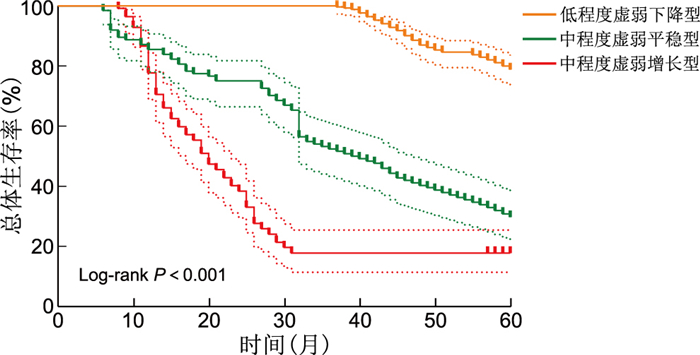
图 1 老年胃癌幸存者的TFI评分轨迹亚型
Figure 1. The TFI score trajectory subtypes of elderly gastric cancer survivors

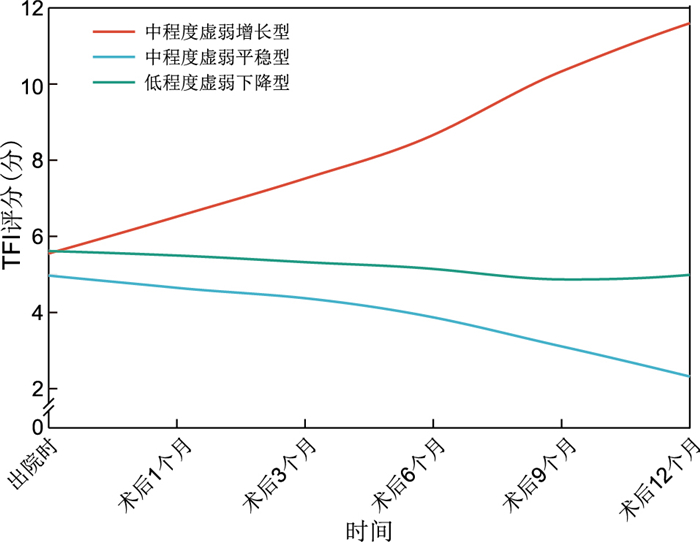
图 2 不同虚弱轨迹组老年胃癌幸存者的生存曲线
Figure 2. Survival curves of elderly gastric cancer survivors in different frailty trajectory groups
表 1 备选GMM中TFI评分拟合结果
Table 1. The fitting results of TFI scores in the alternative GMM
潜在类别个数 LL AIC BIC Class1(%) Class2(%) Class3(%) 1 -5 911.53 11 839.06 11 872.59 100.00 2 -4 029.35 8 090.71 8 157.75 74.59 25.41 3 -3 753.25 7 554.50 7 655.07 25.41 43.85 30.74 注:LL为对数似然比。  下载: 导出CSV
下载: 导出CSV
表 2 不同虚弱轨迹老年胃癌幸存者临床资料比较
Table 2. Comparison of clinical data of elderly gastric cancer survivors with different frailty trajectories
项目 总体(n=488) 低程度虚弱下降型(n=252) 中程度虚弱平稳型(n=124) 中程度虚弱增长型(n=112) 统计量 P值 年龄(x±s, 岁) 71.91±4.10 71.03±3.81 72.69±4.35a 73.03±4.05a 12.790b < 0.001 性别[例(%)] 0.009c 0.995 男性 340(69.7) 176(69.8) 86(69.4) 78(69.6) 女性 148(30.3) 76(30.2) 38(30.6) 34(30.4) BMI(x±s) 20.51±2.03 20.68±2.19 20.49±1.85 20.38±1.83 0.955b 0.386 糖尿病[例(%)] 59(12.1) 19(7.5) 22(17.7)a 18(16.1)a 10.307d 0.006 贫血[例(%)] 30(6.1) 9(3.6) 14(11.3)a 7(6.3) 8.585c 0.014 高血压[例(%)] 190(38.9) 93(36.9) 48(38.7) 49(43.8) 1.532c 0.465 房颤[例(%)] 8(1.6) 2(0.8) 3(2.4) 3(2.7) 2.418c 0.299 低蛋白血症[例(%)] 9(1.8) 1(0.4) 5(4.0)a 3(2.7) 7.111d 0.029 婚姻状况[例(%)] 9.395c 0.009 已婚 421(86.3) 226(89.7) 97(78.2)a 98(87.5) 其他 67(13.7) 26(10.3) 27(21.8)a 14(12.5) 教育程度[例(%)] 1.943d 0.378 小学及以下 251(51.4) 139(55.2) 61(49.2) 51(45.5) 初中 141(28.9) 64(25.4) 39(31.5) 38(33.9) 高中/中专 52(10.7) 26(10.3) 12(9.7) 14(12.5) 大专/本科及以上 44(9.0) 23(9.1) 12(9.7) 9(8.0) 肿瘤分期[例(%)] 3.249d 0.197 Ⅰ期 168(34.4) 94(37.3) 39(31.5) 35(31.3) Ⅱ期 68(13.9) 38(15.1) 18(14.5) 12(10.7) Ⅲ期 252(51.6) 120(47.6) 67(54.0) 65(58.0) 吸烟[例(%)] 173(35.5) 95(37.7) 42(33.9) 36(32.1) 1.227c 0.541 饮酒[例(%)] 325(66.6) 170(67.5) 80(64.5) 75(67.0) 0.333c 0.847 家庭照顾者[例(%)] 8.374c 0.015 主要 114(23.4) 55(21.8) 22(17.7) 37(33.0)a 非主要 374(76.6) 197(78.2) 102(82.3) 75(67.0)a 个人月收入[例(%)] 21.552c < 0.001 < 1 000元 243(49.8) 100(39.7) 77(62.1)a 66(58.9)a ≥1 000元 245(50.2) 152(60.3) 47(37.9)a 46(41.1)a MNA-SF评分(x±s, 分) 8.01±2.82 8.58±2.86 7.83±2.47a 6.91±2.78a 14.636b < 0.001 SSRS评分(x±s, 分) 42.28±10.05 43.66±8.11 41.85±12.55 39.65±10.42a 6.458b 0.002 注:与低程度虚弱下降型比较,aP<0.05。b为F值,c为χ2值, d为U值。
下载: 导出CSV
表 3 中程度虚弱平稳型老年胃癌幸存者影响因素的多因素logistic回归分析
Table 3. Multivariate logistic regression analysis of influencing factors for middle degree weakness and stable condition elderly gastric cancer survivors
变量 B SE Waldχ2 OR(95% CI) P值 年龄 0.102 0.030 11.549 1.108(1.044~1.175) 0.001 糖尿病 0.814 0.363 5.021 2.257(1.107~4.602) 0.025 贫血 1.354 0.470 8.314 3.874(1.543~9.725) 0.004 低蛋白血症 1.932 1.129 2.928 6.902(0.755~63.083) 0.087 已婚 -0.842 0.333 6.397 0.431(0.224~0.827) 0.011 个人月收入≥1 000元 -1.061 0.249 18.199 0.346(0.213~0.564) <0.001 MNA-SF评分 -0.112 0.046 5.848 0.894(0.817~0.979) 0.016
下载: 导出CSV
表 4 中程度虚弱增长型老年胃癌幸存者影响因素的多因素logistic回归分析
Table 4. Multivariate logistic regression analysis of influencing factors for middle-grade weakness-enhanced elderly gastric cancer survivors
变量 B SE Waldχ2 OR(95% CI) P值 年龄 0.139 0.034 16.532 1.149(1.074~1.228) <0.001 糖尿病 0.993 0.420 5.596 2.699(1.186~6.142) 0.018 家庭主要照顾者 0.968 0.301 10.322 2.634(1.459~4.755) 0.001 个人月收入≥1 000元 -1.042 0.265 15.443 0.353(0.210~0.593) <0.001 MNA-SF评分 -0.270 0.053 25.875 0.764(0.688~0.847) <0.001 SSRS评分 -0.055 0.015 13.872 0.946(0.919~0.974) <0.001
下载: 导出CSV
-
[1] 赵萌, 夏勇生, 王子良, 等. ALDH8A1在胃癌组织中的表达及其临床意义[J]. 中华全科医学, 2024, 22(7): 1129-1132, 1255. doi: 10.16766/j.cnki.issn.1674-4152.003582ZHAO M, XIA Y S, WANG Z L, et al. Expression and clinical significance of ALDH8A1 in gastric cancer tissues[J]. Chinese Journal of General Practice, 2024, 22(7): 1129-1132, 1255. doi: 10.16766/j.cnki.issn.1674-4152.003582 [2] MACHLOWSKA J, BAJ J, SITARZ M, et al. Gastric cancer: epidemiology, risk factors, classification, genomic characteristics and treatment strategies[J]. Int J Mol Sci, 2020, 21(11): 4012. DOI: 10.3390/ijms21114012. [3] MIAO X, GUO Y, DING L, et al. A dynamic online nomogram for predicting the heterogeneity trajectories of frailty among elderly gastric cancer survivors[J]. Int J Nurs Stud, 2024, 153: 104716. DOI: 10.1016/j.ijnurstu.2024.104716. [4] LIM H S, LEE B, CHO I, et al. Nutritional and clinical factors affecting weight and fat-free mass loss after gastrectomy in patients with gastric cancer[J]. Nutrients, 2020, 12(7): 1905. DOI: 10.3390/nu12071905. [5] DOODY P, LORD J M, GREIG C A, et al. Frailty: pathophysiology, theoretical and operational definition(s), impact, prevalence, management and prevention, in an increasingly economically developed and ageing world[J]. Gerontology, 2023, 69(8): 927-945. doi: 10.1159/000528561 [6] 程连, 阮金婷, 梁镭, 等. 衰弱评估工具在基层医疗中的应用现状[J]. 中华全科医学, 2024, 22(3): 486-490. doi: 10.16766/j.cnki.issn.1674-4152.003432CHENG L, RUAN J T, LIANG L, et al. Application status of frailty assessment tools in primary care[J]. Chinese Journal of General Practice, 2024, 22(3): 486-490. doi: 10.16766/j.cnki.issn.1674-4152.003432 [7] SUN Y, TIAN Y, CAO S, et al. Multimodal prehabilitation to improve the clinical outcomes of frail elderly patients with gastric cancer: a study protocol for a multicentre randomised controlled trial (GISSG+2201)[J]. BMJ Open, 2023, 13(10): e071714. DOI: 10.1136/bmjopen-2023-071714. [8] DING L, MIAO X, LU J, et al. Comparing the performance of different instruments for diagnosing frailty and predicting adverse outcomes among elderly patients with gastric cancer[J]. J Nutr Health Aging, 2021, 25(10): 1241-1247. doi: 10.1007/s12603-021-1701-8 [9] DING L, MIAO X, JIANG X, et al. Adverse outcomes and health-ecological influencing factors of preoperative frailty among elderly patients with gastric cancer[J]. J Cancer Res Clin Oncol, 2023, 149(10): 7043-7051. doi: 10.1007/s00432-023-04651-z [10] NISHI M, WADA Y, YOSHIKAWA K, et al. Prognostic impact of frailty after gastrectomy in elderly gastric cancer patients[J]. J Med Invest, 2023, 70(3.4): 423-429. doi: 10.2152/jmi.70.423 [11] TAN Z K, TANG W Z, JIA K, et al. Relation between frailty and adverse outcomes in elderly patients with gastric cancer: a scoping review[J]. Ann Med Surg(Lond), 2024, 86(3): 1590-1600. doi: 10.1097/MS9.0000000000001817 [12] JEONG J R, CHOI J W, RYU S Y, et al. Relationship between frailty and mortality after gastrectomy in older patients with gastric cancer[J]. J Geriatr Oncol, 2022, 13(1): 67-73. doi: 10.1016/j.jgo.2021.06.010 [13] SAHIN E, SAHIN K, ULUTAS M E, et al. Calculation of the frailty index and precautions for elderly patients undergoing gastrointestinal cancer surgery[J]. Cureus, 2025, 17(1): e78097. DOI: 10.7759/cureus.78097. [14] 丁玲玉, 蒋小曼, 缪雪怡, 等. 健康生态学视角下老年胃癌患者术前衰弱感知影响因素的质性研究[J]. 中国全科医学, 2023, 26(8): 972-979.DING L Y, JIANG X M, LIAO X Y, et al. Perceived influencing factors of preoperative frailty among elderly patients with gastric cancer from the perspective of health ecology: a qualitative study[J]. Chinese General Practice, 2023, 26(8): 972-979. [15] SHI J, TAO Y, WANG L, et al. Combined effect of diabetes and frailty on mortality among Chinese older adults: a follow-up study[J]. Front Endocrinol(Lausanne), 2023, 13: 1105957. DOI: 10.3389/fendo.2022.1105957. [16] DÜZGÜN G, ÜSTÜNDAǦ S, KARADAKOVAN A. Assessment of frailty in the elderly[J]. Florence Nightingale J Nurs, 2021, 29(1): 2-8. doi: 10.5152/FNJN.2021.414736 [17] HAN D, WANG S K, CUI P, et al. Preoperative nutritional status screened by mna-sf predicts major complications in elderly patients undergoing lumbar fusion surgery[J]. Clin Interv Aging, 2024, 19: 2031-2042. doi: 10.2147/CIA.S481610 [18] ZHANG Q, YU S, LI Q, et al. Preoperative nutritional status in elderly inpatients with gastrointestinal cancer and its linear association with frailty[J]. Nutr Cancer, 2022, 74(4): 1376-1387. doi: 10.1080/01635581.2021.1955284 [19] LEE C T, CHEN M Z, YIP C Y C, et al. Prevalence of anemia and its association with frailty, physical function and cognition in community-dwelling older adults: findings from the HOPE study[J]. J Nutr Health Aging, 2021, 25(5): 679-687. doi: 10.1007/s12603-021-1625-3 [20] 彭心雨, 宋明方, 张婉, 等. 社区老年人社会衰弱现状及影响因素[J]. 护理研究, 2021, 35(19): 3401-3406.PENG X Y, SONG M F, ZHANG W, et al. Status quo and influencing factors of social frailty for the elderly in community[J]. Chinese Nursing Research, 2021, 35(19): 3401-3406. [21] 张圆圆, 张馨月, 陈长香. 不同年龄和衰弱状态下社区老年人身心健康轨迹分析[J]. 重庆医学, 2021, 50(18): 3194-3199.ZHANG Y Y, ZHANG X Y, CHEN C X. Analysis of the developmental trajectory of physical and mental health of the elderly in different age stages and frailty state in urban communities[J]. Chongqing Medicine, 2021, 50(18): 3194-3199. [22] 徐萍, 刘燕玲. 南昌市社区居家老年人衰弱现状与家庭主要照顾者负担的相关性研究[J]. 护理研究, 2022, 36(10): 1791-1797.XU P, LIU Y L. Study on correlation between frailty in community home elderly and burden in main family caregivers in Nanchang city[J]. Chinese Nursing Research, 2022, 36(10): 1791-1797. [23] 刘兰, 马文. 六盘水市社区老年衰弱的发生现状及其影响因素[J]. 贵州医科大学学报, 2024, 49(10): 1477-1483.LIU L, MA W. Study on the situation of senile frailty and its influencing factors in Liupanshui communities[J]. Journal of Guizhou Medical University, 2024, 49(10): 1477-1483. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 6
- HTML全文浏览量: 3
- PDF下载量: 0
- 被引次数: 0
